10-K: Annual report pursuant to Section 13 and 15(d)
Published on March 1, 2018
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
|
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2017
Or
|
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number 033-80623
Achieve Life Sciences, Inc.
(Exact name of the registrant as specified in its charter)
|
Delaware |
|
95-4343413 |
|
(State or other jurisdiction of incorporation or organization) |
|
(I.R.S. Employer Identification No.) |
1001 W. Broadway, Suite 400, Vancouver, British Columbia, V6H 4B1
(Address of principal executive offices, including zip code)
(604) 736-3678
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
Title of Each Class |
|
Name of Exchange on Which Registered |
|
Common Stock, par value $0.001 per share |
|
The NASDAQ Capital Market |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such report), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☒
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
|
☐ |
|
Accelerated filer |
|
☐ |
|
|
|
|
|
|||
|
Non-accelerated filer |
|
☐ |
|
Smaller reporting company |
|
☒ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Emerging growth company |
|
☐ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act.). Yes ☐ No ☒
As of June 30, 2017, the aggregate market value of the registrant’s Common Stock held by non-affiliates of the registrant was $10,680,134. As of March 1, 2018, 12,747,932 shares of the registrant’s Common Stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the Registrant’s Definitive Proxy Statement for its 2018 Annual Meeting of Stockholders (“Proxy Statement”), to be filed within 120 days of the Registrant’s fiscal year ended December 31, 2017, is incorporated by reference into Part III of this Annual Report on Form 10-K
Table of Contents
|
|
|
|
|
||||
|
ITEM 1. |
|
|
3 |
||||
|
ITEM 1A. |
|
|
16 |
||||
|
ITEM 1B. |
|
|
37 |
||||
|
ITEM 2. |
|
|
37 |
||||
|
ITEM 3. |
|
|
37 |
||||
|
ITEM 4. |
|
|
37 |
||||
|
|
|
|
|||||
|
|
|
|
|
||||
|
ITEM 5. |
|
|
38 |
||||
|
ITEM 6. |
|
|
40 |
||||
|
ITEM 7. |
|
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
|
41 |
|||
|
ITEM 7A. |
|
|
51 |
||||
|
ITEM 8. |
|
|
52 |
||||
|
ITEM 9. |
|
CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
|
82 |
|||
|
ITEM 9A. |
|
|
82 |
||||
|
ITEM 9B. |
|
|
82 |
||||
|
|
|
|
|||||
|
|
|
|
|
||||
|
ITEM 10. |
|
|
83 |
||||
|
ITEM 11. |
|
|
83 |
||||
|
ITEM 12. |
|
SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
|
83 |
|||
|
ITEM 13. |
|
CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
|
83 |
|||
|
ITEM 14. |
|
|
83 |
||||
|
|
|
|
|||||
|
|
|
|
|
||||
|
ITEM 15. |
|
|
84 |
||||
2
References in this Form 10-K to “Achieve Life Sciences,” “Achieve,” the “Company,” “we,” “us” or “our” refer to Achieve Life Sciences, Inc. and its wholly owned subsidiaries. The information in this Annual Report on Form 10-K contains certain forward-looking statements, including statements related to clinical trials, regulatory approvals, markets for our products, new product development, capital requirements and trends in our business that involve risks and uncertainties. Our actual results may differ materially from the results discussed in the forward-looking statements. Factors that might cause such a difference include those discussed in “Business,” “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” as well as those discussed elsewhere in this Annual Report on Form 10-K.
OVERVIEW OF OUR BUSINESS AND RECENT DEVELOPMENTS
We are a clinical-stage pharmaceutical company committed to the global development and commercialization of cytisine for smoking cessation. Our focus is to address the global smoking health epidemic, which is a leading cause of preventable death and is responsible for approximately six million deaths annually worldwide.
Cytisine is an established 25-day smoking cessation treatment that has been approved and marketed in Central and Eastern Europe by Sopharma AD for over 20 years under the brand name TabexTM. It is estimated that over 20 million people have used cytisine to help treat nicotine addiction, including over 2,000 patients in investigator-conducted, Phase 3 clinical trials in Europe and New Zealand. Both trials were published in the New England Journal of Medicine in September 2011 and December 2014, respectively.
Cytisine is a naturally occurring, plant-based alkaloid from the seeds of the Laburnum anagyroides plant. Cytisine is structurally similar to nicotine and has a well-defined, dual-acting mechanism of action that is both agonistic and antagonistic. It is believed to aid in smoking cessation by interacting with nicotine receptors in the brain by reducing the severity of nicotine withdrawal symptoms through agonistic binding to nicotine receptors and by reducing the reward and satisfaction associated with smoking through antagonistic properties. The cytisine dosing schedule reflects that of an anti-addiction medication, with downward dose titration over a period of 25 days.
In late June 2017, we filed our Investigational New Drug, or IND, application for cytisine with the United States Food and Drug Administration, or FDA, which included National Center for Complementary and Integrative Health, or NCCIH, sponsored non-clinical studies. The IND was accepted in late July 2017.
In August 2017, we initiated a study evaluating the effect of food on the bioavailability of cytisine in normal healthy volunteers. We completed the food effect study and announced the results in November of 2017 demonstrating similar bioavailability of cytisine in fed and fasted subjects.
In October 2017, we initiated a study assessing the repeat-dose Pharmacokinetics, or PK, and Pharmacodynamics, or PD, effects of 1.5mg and 3mg cytisine in 36 healthy volunteer smokers aged 18-65 years when administered over the standard 25-day course of treatment. Preliminary results on 24 smokers were announced in February 2018. The PK results indicated expected increases in plasma concentration with higher doses of cytisine. Smokers in the study were not required to have a designated or predetermined quit date, however, 58% of the subjects in the trial achieved biochemically verified smoking abstinence by day 26. Half (6/12) of the subjects on the 1.5mg arm and 67% (8/12) of the subjects on the 3.0mg arm achieved abstinence on day 26. Subjects who did not achieve abstinence had a significant reduction in number of daily cigarettes smoked by day 26. The adverse events observed were mostly mild with transient headaches as the most commonly reported event. No serious adverse events were observed in the study.
In December 2017, we submitted a meeting request to hold a pre-Phase 3 meeting with the FDA to review our Phase 3 program and overall development plans for cytisine. We received confirmation from the FDA for a meeting date in the second quarter of 2018. We intend to commence a Phase 3 clinical program in mid-2018, subject to FDA guidance and the availability of capital. In addition to the Phase 3 program, we expect to run additional supportive clinical studies including, but not limited to urinary excretion of cytisine, renal impairment and QT interval prolongation studies as well as supportive New Drug Application, or NDA, non-clinical chronic toxicity and carcinogenicity studies.
While third party trials of cytisine have been conducted that may inform future Company-sponsored clinical trials, we have not yet conducted any large scale company-sponsored clinical trials for cytisine in the United States or any other jurisdiction.
3
Our management team has significant experience in growing emerging companies focused on the development of under-utilized pharmaceutical compounds to meet unmet medical needs. We intend to use this experience to develop and ultimately commercialize cytisine either directly or via strategic collaborations.
Recent Corporate History
On August 1, 2017, OncoGenex Pharmaceuticals, Inc., or OncoGenex, completed a transaction, or the Arrangement, with Achieve Life Science, Inc., or Achieve, as contemplated by the Merger Agreement between Achieve and OncoGenex dated January 5, 2017, or the Merger Agreement. Under the terms of the Merger Agreement, OncoGenex changed its name to Achieve Life Sciences, Inc., instituted an one-for-eleven reverse stock split, issued 8,210,118 shares of its common stock (after accounting for the elimination of resulting fractional shares) in exchange for all of the outstanding preferred shares, common shares and convertible debentures of Achieve, and as a result Achieve became a wholly-owned subsidiary of OncoGenex, and is listed on the Nasdaq Capital Market under the ticker symbol ACHV. More information concerning the Arrangement is contained in our Current Report on Form 8-K filed on August 2, 2017 and our Amendment No. 3 to the Registration Statement on Form S-4/A filed with the SEC on June 6, 2017.
The financial results account for the Arrangement between OncoGenex and Achieve as a reverse merger, whereby Achieve is deemed to be the acquiring entity from an accounting perspective. Our consolidated results of operations for the year ended December 31, 2017 include the results of operations of only Achieve for the time period of January 1, 2017 through August 1, 2017 and include the results of the combined company following the completion of the Arrangement on August 1, 2017. The consolidated results of operations for the years ended December 31, 2016 and December 31, 2015 include only the consolidated results of operations of Achieve and do not include historical results of OncoGenex. This treatment and presentation is in accordance with ASC 805, “Business Combinations”. Information relating to the number of shares, price per share and per share amounts of common stock are presented on a post- reverse stock split basis, as a reverse stock split in the ratio of one-for-eleven was effected in connection with the Arrangement.
We have no products approved for commercial sale and have not generated any revenue from product sales to date. We have never been profitable and have incurred operating losses in each year since inception. Our net loss was $10.6 million, $1.2 million and $0.8 million for years end December 31, 2017, 2016 and 2015, respectively. As of December 31, 2017, we had an accumulated deficit of $12.7 million, cash and cash equivalents balance of $5.3 million and a positive working capital balance of $3.7 million. Substantially all of our operating losses resulted from expenses incurred from general and administrative costs associated with our operations and research and development costs from our clinical development programs.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our ability to obtain additional financing. We expect to incur significant expenses and increasing operating losses for at least the next several years as we continue our clinical development of, and seek regulatory approval for, cytisine and add personnel necessary to operate as a public company with an advanced clinical candidate. We expect that our operating losses will fluctuate significantly from quarter to quarter and year to year due to timing of clinical development programs and efforts to achieve regulatory approval. Without additional funds, we may be forced to delay, scale back or eliminate some of our research and development activities or other operations and potentially delay product development in an effort to provide sufficient funds to continue our operations. If any of these events occur, our ability to achieve our development and commercialization goals would be adversely affected.
Our current capital resources are insufficient to fund our planned operations for the next 12 months. We will continue to require substantial additional capital to continue our clinical development activities. Accordingly, we will need to raise substantial additional capital to continue to fund our operations, from the sale of our securities, partnering arrangements or other financing transactions in order to finance the commercialization of our product candidates. The amount and timing of our future funding requirements will depend on many factors, including the pace and results of our clinical development efforts. Failure to raise capital as and when needed, on favorable terms or at all, will have a negative impact on our financial condition and our ability to develop our product candidate.
The accompanying financial results have been prepared assuming we will continue to operate as a going concern, which contemplates the realization of assets and liabilities and commitments in the normal course of business. The financial results do not include any adjustments to the amounts and classification of assets and liabilities that might be necessary should we be unable to continue as a going concern. Such adjustments could be material.
Product Candidate Overview
Our product candidate, cytisine, is a naturally occurring plant-based alkyloid from the seeds of the Laburnum anagyroides plant. Cytisine is a smoking cessation aid that interacts with nicotine receptors in the brain and is believed to help reduce the severity of nicotine withdrawal symptoms and the reward and satisfaction associated with smoking.
4
Cytisine is an established 25-day smoking cessation treatment that has been approved and marketed in Central and Eastern Europe by a third party for over 20 years under the brand name TabexTM. It is estimated that over 20 million people have used cytisine to help treat nicotine addiction, including over 2,000 patients in investigator-conducted, Phase 3 clinical trials in Europe and New Zealand. Both trials were published in the New England Journal of Medicine in September 2011 and December 2014.
Apatorsen
In August 2017, we discontinued further development of apatorsen. We provided a notice of discontinuance to our former development partners for apatorsen, Ionis Pharmaceuticals, Inc., or Ionis, and a letter of termination to the University of British Columbia, or UBC, notifying them that we have discontinued development of apatorsen resulting in termination of all licensing agreements related to this product candidate. We believe that all financial obligations, other than continuing mutual indemnification obligations and our requirement to pay for out-of-pocket patent expenses incurred up to the date of termination and for abandoning the apatorsen patents and patent applications, under all apatorsen related agreements with Ionis and UBC, are no longer owed and no further payments are due.
OUR PRODUCT CANDIDATE - CYTISINE
Overview of Cytisine
Our product candidate, cytisine, is a naturally occurring plant-based alkyloid from the seeds of the Laburnum anagyroides plant. Cytisine is a smoking cessation aid that interacts with nicotine receptors in the brain and is believed to help reduce the severity of nicotine withdrawal symptoms and the reward and satisfaction associated with smoking.
Cytisine is an established 25-day smoking cessation treatment that has been approved and marketed in Central and Eastern Europe by a third party for over 20 years under the brand name TabexTM. It is estimated that over 20 million people have used cytisine to help treat nicotine addiction, including over 2,000 patients in investigator-conducted, Phase 3 clinical trials in Europe and New Zealand. Both trials were published in the New England Journal of Medicine in September 2011 and December 2014. TabexTM is currently marketed in a number of countries in Central and Eastern Europe, as well as in other geographic regions, as Over-the-Counter drug, or OTC.
Cytisine Mechanism of Action
Cytisine is a partial agonist that binds with high affinity to the alpha-4 beta-2, or a4b2, nicotinic acetylcholine receptors in the brain. Through dual-acting partial agonist/partial antagonist activity, cytisine is believed to help reduce nicotine cravings, withdrawal symptoms and reward and satisfaction associated with smoking. The a4b2 nicotinic receptor is a well-understood target in addiction. When nicotine binds to this receptor, it causes dopamine to be released in the mid brain, reinforcing the dopamine reward system. This receptor has been implicated in the development and maintenance of nicotine dependence. Cytisine is believed to act as a partial agonist at the a4b2 nicotinic receptor, preventing nicotine from binding and releasing dopamine.
Cytisine Opportunity
We have an exclusive license and supply agreement with Sopharma for the development and commercialization of cytisine outside of Sopharma’s territory, which consists of certain countries in Central and Eastern Europe, Scandinavia, North Africa, the Middle East and Central Asia, as well as Vietnam. We intend to develop and commercialize cytisine in the United States and intend thereafter to target other markets outside of Sopharma’s territory, such as Western Europe, Japan, Australasia, Southeast Asia and Latin and South America.
We are developing cytisine as an aid to smoking cessation and nicotine dependence to address the limitations of both prescription drugs and OTC products. We believe that a substantial market exists in the United States, European Union, or EU, and the rest of the world for a safe and effective smoking cessation treatment. Increasingly constrained healthcare budgets have focused government attention on drug pricing, which we believe cytisine can address by serving as a cost-effective alternative to existing treatments, with the potential for better efficacy than nicotine replacement therapies, or NRTs, and a potentially superior side effect profile than existing prescription smoking cessation products. Our goal is to obtain approval from the FDA and from other regulatory agencies for the sale and distribution of cytisine in the United States and subsequently to other countries outside of Sopharma’s territory.
We have met with the United States Food and Drug Administration, or FDA, and with other national regulatory authorities in Europe to identify the steps required for the approval of cytisine. The FDA requested results from non-clinical studies, additional human
5
pharmacokinetic studies and adequate demonstration of safety and efficacy from randomized, placebo-controlled, Phase 3 clinical trials.
The non-clinical studies requested by the FDA have been sponsored and completed by the National Center for Complementary and Integrative Health, or NCCIH, division of the U.S. National Institutes of Health, in addition to the National Cancer Institute. In July 2017, we filed our Investigational New Drug, or IND, application for cytisine with the FDA, which included NCCIH sponsored non-clinical studies. The IND was accepted in late July 2017.
In August 2017, we initiated a study evaluating the effect of food on the bioavailability of cytisine in normal healthy volunteers. We completed the food effect study and announced the results in November of 2017 demonstrating similar bioavailability of cytisine in fed and fasted subjects.
In October 2017, we initiated a study assessing the repeat-dose Pharmacokinetics, or PK, and Pharmacodynamics, or PD, effects of 1.5mg and 3mg cytisine in 36 healthy volunteer smokers aged 18-65 years when administered over the standard 25-day course of treatment. Preliminary results on 24 smokers were announced in February 2018. The PK results indicated expected increases in plasma concentration with higher doses of cytisine. Smokers in the study were not required to have a designated or predetermined quit date, however, 58% of the subjects in the trial achieved biochemically verified smoking abstinence by day 26. Half (6/12) of the subjects on the 1.5mg arm and 67% (8/12) of the subjects on the 3.0mg arm achieved abstinence on day 26. Subjects who did not achieve abstinence had a significant reduction in number of daily cigarettes smoked by day 26. The adverse events observed were mostly mild with transient headaches as the most commonly reported event. No serious adverse events were observed in the study.
In December 2017, we initiated a number of in vitro drug to drug interaction studies of cytisine and expect data from these studies to be available in the first half of 2018. Also in December 2017, we submitted a meeting request to hold a pre-Phase 3 meeting with the FDA to review our Phase 3 program and overall development plans for cytisine. We received confirmation from the FDA for a meeting date in the second quarter of 2018. We intend to commence a Phase 3 clinical program in mid-2018, subject to FDA guidance and the availability of capital. In addition to the Phase 3 program, we expect to run additional supportive clinical studies including, but not limited to urine excretion, renal impairment and QT interval prolongation studies as well as supportive NDA non-clinical chronic toxicity and carcinogenicity studies.
While third party trials of cytisine have been conducted that may inform future Company-sponsored clinical trials, we have not yet conducted any large scale company-sponsored clinical trials for cytisine in the United States or any other jurisdiction.
Cytisine Clinical Trials
Cytisine has been tested in two large, randomized Phase 3 clinical trials conducted according to Good Clinical Practice, or GCP, in more than 2,000 participants. The objective was to evaluate the efficacy and safety of cytisine according to current clinical development standards.
TASC Trial
The Tabex Smoking Cessation, or TASC, trial, was sponsored by the UK Centre for Tobacco Control Studies and evaluated cytisine versus placebo in 740 primarily moderate-to-heavy smokers treated for 25 days in a single center in Warsaw, Poland. The primary outcome measure was sustained, biochemically verified smoking abstinence for 12 months after the end of treatment. The TASC trial was conceived by Professor Robert West (Department of Epidemiology and Public Health, University College London) and was funded by the a grant from the National Prevention Research Initiative, including contributions from Cancer Research UK, Medical Research Council, United Kingdom Department of Health and others. We, through our partner Sopharma, provided the study drug used in this trial.
The results of the TASC trial were published in the New England Journal of Medicine in September 2011. The rate of sustained 12-month abstinence was 8.4% in the cytisine arm as compared with 2.4% in the placebo group (p=0.001). These results showed that cytisine was 3.4 times more likely than a placebo to help participants stop smoking and remain non-smokers for one year. The rate of sustained 6-month abstinence was 10.0% in the cytisine arm as compared with 3.5% in the placebo group (p<0.001). Cytisine was well tolerated with a slight but significant increase in combined gastrointestinal adverse events (upper abdominal pain, nausea, dyspepsia and dry mouth; cytisine 51/370 (13.8%) and placebo 30/370 (8.1%). The safety profile of cytisine was similar to that of a placebo with no other significant differences in the rate of side effects in the two trial arms.
A summary of adverse events reported in 10 or more subjects in the TASC trial is included in the table below.
6
TASC - Adverse Events Reported by 10 or More Study Participants(1)
|
|
|
|
|
|
|
|
Event |
|
Cytisine (N=370) |
|
Placebo (N=370) |
|
|
|
percent (number) |
|
|||
|
Any gastrointestinal event |
|
13.8% (51) |
|
8.1% (30) |
|
|
Upper abdominal pain |
|
3.8 (14) |
|
3.0 (11) |
|
|
Nausea |
|
3.8 (14) |
|
2.7 (10) |
|
|
Dyspepsia |
|
2.4 (9) |
|
1.1 (4) |
|
|
Dry mouth |
|
2.2 (8) |
|
0.5 (2) |
|
|
Any psychiatric event |
|
4.6% (17) |
|
3.2% (12) |
|
|
Dizziness |
|
2.2 (8) |
|
1.1 (4) |
|
|
Somnolence |
|
1.6 (6) |
|
1.1 (4) |
|
|
Any nervous system event |
|
2.7% (10) |
|
2.4% (9) |
|
|
Headache |
|
1.9 (7) |
|
2.2 (8) |
|
|
Skin and subcutaneous tissue |
|
1.6% (6) |
|
1.4% (5) |
|
|
(1) |
The incidence of events was analyzed according to the Medical Dictionary for Regulatory Activities System Organ Class, or SOC, categorization and preferred terms. Participants who reported more than one event in a system category were counted only once for the category. SOC categories for other events (those reported by fewer than 10 participants) were as follows: general (five events within cytisine and five with placebo), cardiac (four with cytisine and two with placebo), musculoskeletal and connective tissue (three with cytisine and three with placebo), infections (one with placebo), immune system (one with placebo) and metabolism and nutrition (one with placebo). |
CASCAID Trial
The second Phase 3 trial, the Cytisine As a Smoking Cessation Aid, or CASCAID, non-inferiority trial, was an open-label trial that randomized 1,310 adult daily smokers. Patients were randomized to receive either cytisine for 25 days or NRT for 8 weeks. Both treatment groups were offered low intensity telephone behavioral support during trial treatment. The primary outcome measure was continuous self-reported abstinence from smoking one month after quit date. The CASCAID trial was conducted by the Health Research Council of New Zealand. We, through our partner Sopharma, provided the cytisine in form of commercial TabexTM used in this trial.
The results of the CASCAID trial, which were published in the New England Journal of Medicine in December 2014, showed that cytisine was superior to NRT for smoking cessation and, specifically, that cytisine was 1.43 times more likely than nicotine gums or patches to help participants stop smoking and remain non-smokers for six months. The rate of continuous one-month abstinence was 40% in the cytisine arm as compared with 31% in the NRT arm (p<0.001). A secondary outcome included the rate of continuous six-month abstinence which was 22% in the cytisine arm as compared with 15% in the NRT arm (p=0.002). Cytisine was generally well tolerated, although self-reported adverse events were slightly higher in the cytisine arm compared with the NRT arm. The most frequent adverse events for cytisine were nausea and vomiting (30/665 (4.6%)) and sleep disorders (28/665 (4.2%)). Reports of these same adverse events in the NRT arm were as follows: nausea and vomiting (2/655 (0.3%)) and sleep disorders (2/655 (0.3%)).
A summary of adverse events reported in subjects in the CASCAID trial is included in the table below.
CASCAID - Summary of All-Cause Adverse Events
|
|
|
|
|
|
|
|
|
|
|
|
|
Event |
|
Cytisine (N=655) |
|
|
NRT (N=655) |
|
|
|||
|
|
percent (number) |
|
|
|||||||
|
Participants with any adverse event no. (%) |
|
|
31% (204) |
|
|
|
20% (134) |
|||
|
Adverse events — no. |
|
|
|
|
|
|
|
|||
|
Any |
|
|
44% (288) |
|
|
|
27% (174) |
|||
|
In those who complied with treatment(1) |
|
|
25 (161) |
|
|
|
17 (113) |
|||
|
In those who did not comply with treatment |
|
|
19 (127) |
|
|
|
9 (61) |
|||
|
Participants with serious adverse event — no. (%) |
|
|
7% (45) |
|
|
|
39 (6%) |
|||
|
Serious adverse events — no.(2)(3) |
|
|
9% (56) |
|
|
|
7 (45) |
|||
7
|
|
|
0.2 (1) |
|
|
|
0.2 (1) |
||||
|
Life-threatening events |
|
|
0 |
|
|
|
0.2 (1)5 |
|||
|
Hospitalizations |
|
|
3 (18) |
|
|
|
3 (18) |
|||
|
Otherwise medically important events |
|
|
6 (37) |
|
|
|
4 (25) |
|||
|
Severity of all adverse events — no.(4) |
|
|
|
|
|
|
|
|||
|
Mild |
|
|
21% (139) |
|
|
|
12% (78) |
|||
|
Moderate |
|
|
17 (111) |
|
|
|
12 (77) |
|||
|
Severe |
|
|
6 (38) |
|
|
|
3 (19) |
|||
|
Most frequent adverse events — no.(5) |
|
|
|
|
|
|
|
|||
|
Nausea and vomiting |
|
|
5% (30) |
|
|
|
0.3% (2) |
|||
|
Sleep disorders |
|
|
4 (28) |
|
|
|
0.3 (2) |
|||
|
(1) |
In the cytisine group, compliance was defined as having taken 80% or more of the required number of tablets within 1 month after the quit date (i.e., 80 or more tablets). In the NRT group, compliance was defined as having used NRT at 1 week and 1 month after the quit date. It was assumed that participants with missing data were not compliant. |
|||||||||
|
(2) |
A serious event was defined as death, a life-threatening event, an event requiring hospitalization, or otherwise medically important event (i.e., the event does not belong in any of the other categories but may jeopardize the patient and may require medical or surgical intervention to prevent the occurrence of one or more other serious events). |
|||||||||
|
(3) |
The categories are mutually exclusive. |
|||||||||
|
(4) |
The severity of events was not medically verified. |
|||||||||
|
(5) |
The list of most frequent adverse events excludes signs and symptoms of cold and influenza. Adverse events were categorized in accordance with the International Statistical Classification of Diseases and Related Health Problems , Tenth Revision (ICD-10), Australian Modification. |
|||||||||
Safety Reporting
As cytisine has been marketed in Central and Eastern Europe for over 20 years, substantial safety reporting exists for cytisine including over 15 million cases. The most recent periodic safety update report, PSUR, submitted to the European authorities by Sopharma in 2016 did not contain new safety signals with cytisine.
OVERVIEW OF MARKET AND TREATMENT
Overview of the Tobacco Epidemic
The NIH and the World Health Organization, or WHO, estimated in January 2017 that approximately 1.1 billion people globally are smokers and that 6 million people die annually from diseases related to tobacco use including 600,000 from passive smoke. This figure is projected to grow to 8 million by 2030. Tobacco use is estimated to cause 12% of deaths among persons aged 30 years and over worldwide, including deaths from cancer, diabetes, cardiovascular disease and lung diseases such as tuberculosis and lower respiratory tract infections. According to the American Cancer Society, smoking is a direct cause of approximately 80% of lung cancer deaths and is linked to 30% of all cancers.
The U.S. Centers for Disease Control, or CDC, estimate that in 2015 approximately 15.1% of all U.S. adults (36.5 million people) were cigarette smokers. Smoking remains the single largest preventable cause of death worldwide and in the United States.
CDC estimates that the annual cost of smoking related illnesses in the United States is more than $300 billion annually in direct medical care and lost productivity. Over 16 million people in the United States are living with a disease caused by smoking. Smoking causes cancer, heart disease, stroke, lung diseases, diabetes and chronic obstructive pulmonary disease, or COPD, which includes emphysema and chronic bronchitis. Smoking also increases risk for tuberculosis, certain eye diseases and problems of the immune system, including rheumatoid arthritis.
Tobacco smoking is highly addictive and research suggests that nicotine may be as addictive as heroin, cocaine or alcohol. The CDC estimates that more people are addicted to nicotine than any other drug and report that nearly 70% of smokers desire to quit and 55% make a quit attempt each year. Despite the high number of attempts, only about 4% to 7% of people are successful in their quit attempt each year.
The Global Smoking Cessation Market
8
Coherent Market Insights Report “Smoking Cessation and Nicotine De-addiction Products Market, 2016-2017” estimated that global revenues for smoking cessation and nicotine de-addiction products in 2016 was approximately $12.8 billion including NRT, e-cigarettes and drug therapy. In 2017, in the U.S. alone, sales for NRT and drug therapy were estimated to be $3.8 billion and is expected to grow to $5.7 billion by 2024.
Two prescription oral treatments for smoking cessation are currently available in the United States: Chantix® (varenicline) marketed by Pfizer and Zyban ® (bupropion) marketed by GlaxoSmithKline (as well as generic manufacturers). Both of these prescription treatments have been proven effective in aiding smoking cessation, however, both are also associated with significant side effects. Chantix’s labeling indicates elevated instances of nausea, abnormal dreams, constipation, flatulence and vomiting may be experienced by Chantix-treated patients compared to placebo-treated patients, and Zyban’s labeling discloses potential adverse reactions including insomnia, rhinitis, dry mouth, dizziness, nervous disturbance, anxiety, nausea, constipation, arthralgia and seizures.
The vast majority of OTC smoking cessation aids are NRTs. NRTs come in many forms, including gums, lozenges and patches, and although they are marketed at a lower price point, they have been shown to be less effective than prescription drugs. For example, a Cochrane Group independent database review of nicotine receptor partial agonists published in 2016 compared varenicline (Chantix) with a number of NRTs and found that varenicline appeared to be more effective than the NRTs.
LICENSE & SUPPLY AGREEMENTS
Sopharma AD
In 2009 and 2010, we entered into a license agreement, or the Sopharma License Agreement, and a supply agreement, or the Sopharma Supply Agreement, with Sopharma, AD, or Sopharma. Pursuant to the Sopharma License Agreement, we were granted access to all available manufacturing, efficacy and safety data related to cytisine, as well as a granted patent in several European countries including Germany, France and Italy related to new oral dosage forms of cytisine providing enhanced stability. Additional rights granted under the Sopharma License Agreement include the exclusive use of, and the right to sublicense, the trademark Tabex in all territories—other than certain countries in Central and Eastern Europe, Scandinavia, North Africa, the Middle East and Central Asia, as well as Vietnam, where Sopharma or its affiliates and agents already market Tabex—in connection with the marketing, distribution and sale of products. Under the Sopharma License Agreement, we agreed to pay a nonrefundable license fee. In addition, we agreed to make certain royalty payments equal to a mid-teens percentage of all net sales of Tabex branded products in our territory during the term of the Sopharma License Agreement, including those sold by a third party pursuant to any sublicense which may be granted by us. We have agreed to cooperate with Sopharma in the defense against any actual or threatened infringement claims with respect to Tabex. Sopharma has the right to terminate the Sopharma License Agreement upon the termination or expiration of the Sopharma Supply Agreement. The Sopharma License Agreement will also terminate under customary termination provisions including bankruptcy or insolvency and material breach. To date, we have paid Sopharma $10 pursuant to the Sopharma License Agreement.
A cross-license exists between us and Sopharma whereby we grant to Sopharma rights to any patents or patent applications or other intellectual property rights filed by us in Sopharma territories.
On May 14, 2015, we and Sopharma entered into an amendment to the Sopharma License Agreement. Among other things, the amendment to the Sopharma License Agreement reduced the royalty payments payable by us to Sopharma from a percentage in the mid-teens to a percentage in the mid-single digits and extended the term of the Sopharma License Agreement until May 26, 2029.
On July 28, 2017, we and Sopharma entered into the amended and restated Sopharma Supply Agreement. Pursuant to the amended and restated Sopharma Supply Agreement, we will exclusively purchase all of our cytisine from Sopharma, Sopharma agrees to exclusively supply all such cytisine requested by us, for territories as detailed in the licensing agreement, and we extended the term to 2037. In addition, we will have full access to the cytisine supply chain and Sopharma will manufacture sufficient cytisine to meet a forecast for a specified demand of cytisine for the five years commencing shortly after the commencement of the agreement, with the forecast to be updated regularly thereafter. We and Sopharma may terminate the Sopharma Supply Agreement in the event of the other party’s material breach or bankruptcy or insolvency.
University of Bristol
In July 2016, we entered into a license agreement with the University of Bristol, or the University of Bristol License Agreement. Under the University of Bristol License Agreement, we received exclusive and nonexclusive licenses from the University of Bristol to certain patent and technology rights resulting from research activities into cytisine and its derivatives, including a number of patent applications related to novel approaches to cytisine binding at the nicotinic receptor level. Any patents issued in connection with these applications would be scheduled to expire on February 5, 2036 at the earliest.
9
In consideration of rights granted by the University of Bristol, we paid a nominal license fee and agreed to pay amounts of up to $3.2 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the University of Bristol License Agreement. Additionally, if we successfully commercialize product candidates subject to the University of Bristol License Agreement, we are responsible for royalty payments in the low-single digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products.
On January 22, 2018, we and the University of Bristol entered into an amendment to the University of Bristol License Agreement. Pursuant to the amended University of Bristol License Agreement we received exclusive rights for all human medicinal uses of cytisine across all therapeutic categories from the University of Bristol from research activities into cytisine and its derivatives. In consideration of rights granted by the amended University of Bristol License Agreement, we agreed to pay an initial amount of $37,500 upon the execution of the amended University of Bristol License Agreement, and additional amounts of up to $1.7 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the amended University of Bristol License Agreement, in addition to amounts under the original University of Bristol License Agreement of up to $3.2 million in the aggregate, tied to specific financing, development and commercialization milestones. Additionally, if we successfully commercialize any product candidate subject to the amended University of Bristol License Agreement or to the original University of Bristol License Agreement, we will be responsible, as provided in the original University of Bristol License Agreement, for royalty payments in the low-single digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products. To date, we have paid the University of Bristol $50,000 pursuant to the University of Bristol License Agreement.
Unless otherwise terminated, the University of Bristol License Agreement will continue until the earlier of July 2036 or the expiration of the last patent claim subject to the University of Bristol License Agreement. We may terminate the University of Bristol License Agreement for convenience upon a specified number of days’ prior notice to the University of Bristol. The University of Bristol License Agreement will terminate under customary termination provisions including bankruptcy or insolvency or its material breach of the agreement. Under the terms of the University of Bristol License Agreement, we had provided 100 grams of cytisine to the University of Bristol as an initial contribution. To date, we have not paid any further sums to the University of Bristol pursuant to the University of Bristol License Agreement.
Summary of Milestone Obligations by Product Candidate
The following table sets forth the milestones that we may be required to pay to third parties under the license agreements described above. As described above, we will also be required to pay certain revenue-based royalties with respect to our product candidate.
|
Milestone Obligations to Third Parties |
|
Amount Payable |
|
University of Bristol |
|
Up to $4,837,500 (1) |
|
(1) |
Payable in connection with specific financing, development and commercialization milestones. |
GOVERNMENT REGULATIONS
We are heavily regulated in most of the countries in which we operate In the United States, the principal regulating authority is the FDA. The FDA regulates the safety and efficacy of product candidates and research, quality, manufacturing processes, product approval and promotion, advertising and product labeling. In the EU, the European Medicines Agency, or EMA, and national regulatory agencies regulate the scientific evaluation, supervision and safety monitoring of product candidates, and over-see the procedures for approval of drugs for the EU and European Economic Area countries. In Japan, the Pharmaceuticals and Medical Devices Agency is involved in a wide range of regulatory activities, including clinical trials, approvals, post-marketing reviews and pharmaceutical safety. Similar regulations exist in most other countries, and in many countries the government also regulates prices. Health authorities in many middle and lower income countries require marketing approval by a recognized regulatory authority, such as the FDA or EMA, before they begin to conduct their application review process and/or issue their final approval.
United States
We intend to focus initially on clinical development of cytisine in the United States. It is anticipated that cytisine tablets would receive a minimum five years of data exclusivity under the Drug Price Competition and Patent Term Restoration Act, also known as the Hatch-Waxman Act.
Before a new pharmaceutical product may be marketed in the United States, the FDA must approve an NDA, for a new drug. The steps required before the FDA will approve an NDA generally include non-clinical studies followed by multiple stages of clinical
10
trials conducted by the trial sponsor; sponsor submission of the NDA application to the FDA for review; the FDA’s review of the data to assess the drug’s safety and effectiveness; and the FDA’s inspection of the facilities where the product will be manufactured.
As a condition of product approval, the FDA may require a sponsor to conduct post-marketing clinical trials, known as Phase 4 trials, and surveillance programs to monitor the effect of the approved product. The FDA may limit further marketing of a product based on the results of these post-market trials and programs. Any modifications to a drug, including new indications or changes to labeling or manufacturing processes or facilities, may require the submission and approval of a new or supplemental NDA before the modification can be implemented, which may require that we generate additional data or conduct additional non-clinical studies and clinical trials. Our ongoing manufacture and distribution of drugs is subject to continuing regulation by the FDA, including recordkeeping requirements, reporting of adverse experiences associated with the product, and adherence to current Good Manufacturing Practices, or cGMPs, which regulate all aspects of the manufacturing process. We are also subject to numerous regulatory requirements relating to the advertising and promotion of drugs, including, but not limited to, standards and regulations for direct-to-consumer advertising. Failure to comply with the applicable regulatory requirements governing the manufacture and marketing of our products may subject us to administrative or judicial sanctions, including warning letters, product recalls or seizures, injunctions, fines, civil penalties and/or criminal prosecution.
Sales and Marketing. The marketing practices of U.S. pharmaceutical companies are generally subject to various federal and state healthcare laws that are intended to prevent fraud and abuse in the healthcare industry and protect the integrity of government healthcare programs. These laws include anti-kickback laws and false claims laws. Anti-kickback laws generally prohibit a biopharmaceutical or medical device company from soliciting, offering, receiving or paying any remuneration to generate business, including the purchase or prescription of a particular product. False claims laws generally prohibit anyone from knowingly and willingly presenting, or causing to be presented, any claims for payment for reimbursed drugs or services to third-party payors (including Medicare and Medicaid) that are false or fraudulent. Although the specific provisions of these laws vary, their scope is generally broad and there may not be regulations, guidance or court decisions that apply the laws to any particular industry practices, including the marketing practices of pharmaceutical and medical device companies. Violations of fraud and abuse laws may be punishable by criminal or civil sanctions and/or exclusion from federal health care programs (including Medicare and Medicaid). The U.S. federal government and various states have also enacted laws to regulate the sales and marketing practices of pharmaceutical or medical device companies. These laws and regulations generally limit financial interactions between manufacturers and health care providers; require disclosure to the federal or state government and public of such interactions; and/or require the adoption of compliance standards or programs. Many of these laws and regulations contain ambiguous requirements or require administrative guidance for implementation. Given the lack of clarity in laws and their implementation, our activities could be subject to penalties under the pertinent laws and regulations.
Pricing and Reimbursement. Pricing for our pharmaceutical products will depend in part on government regulation. We will likely be required to offer discounted pricing or rebates on purchases of pharmaceutical products under various federal and state healthcare programs, such as the Medicaid Drug Rebate Program, the “federal ceiling price” drug pricing program, the 340B drug pricing program and the Medicare Part D Program. We will also be required to report specific prices to government agencies under healthcare programs, such as the Medicaid Drug Rebate Program and Medicare Part B. The calculations necessary to determine the prices reported are complex and the failure to report prices accurately may expose us to penalties.
In the United States, Medicaid currently covers all smoking cessation products including Chantix and Zyban. In March 2010, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively, the Health Care Reform Law, was passed, which substantially changes the way health care is financed by both governmental and private insurers, and significantly impacts the U.S. pharmaceutical industry. Section 2502 of the Patient Protection and Affordable Care Act, or ACA, specifies that tobacco cessation medications will be removed from the list of optional medications and required for inclusion in states’ prescription drug benefit. On May 2, 2014 the Department of Health and Human Services, or HHS, provided guidance into insurance coverage policy that health plans would be in compliance if they cover, among other items, screening for tobacco use, individual, group and phone counseling, all FDA approved tobacco cessation medications (both prescription and OTC) when prescribed by a healthcare provider, at least two quit attempts per year, four sessions of counseling and 90 days of treatment, with no cost sharing (co-pay) required.
Government and private third-party payers routinely seek to manage utilization and control the costs of our products. For example, the majority of states use preferred drug lists to restrict access to certain pharmaceutical products under Medicaid. Given certain states’ current and potential ongoing fiscal crises, a growing number of states are considering a variety of cost-control strategies, including capitated managed care plans that typically contain cost by restricting access to certain treatments.
11
Healthcare Reform. The U.S. and state governments continue to propose and pass legislation designed to regulate the healthcare industry. In March 2010, the U.S. Congress enacted the ACA, which included changes that significantly affected the pharmaceutical industry, such as:
|
|
• |
|
increasing drug rebates paid to state Medicaid programs under the Medicaid Drug Rebate Program for brand name and generic prescription drugs and extending those rebates to Medicaid managed care; |
|
|
• |
|
Requiring pharmaceutical manufacturers to provide discounts on brand name prescription drugs sold to Medicare beneficiaries whose prescription drug costs cause the beneficiaries to be subject to the Medicare Part D coverage gap; and |
|
|
• |
|
Imposing an annual fee on manufacturers and importers of brand name prescription drugs reimbursed under certain government programs, including Medicare and Medicaid.
|
The ACA includes provisions designed to increase the number of Americans covered by health insurance. Specifically, since 2014, the ACA has required most individuals to maintain health insurance coverage or potentially to pay a penalty for noncompliance and has offered states the option of expanding Medicaid coverage to additional individuals. Additionally, policy efforts designed specifically to reduce patient out-of-pocket costs for medicines could result in new mandatory rebates and discounts or other pricing restrictions. Adoption of other new legislation at the federal or state level could further affect demand for, or pricing of, our products.
On January 20, 2017, President Donald Trump issued an Executive Order to initiate the repeal of the Health Care Reform Law and we expect that additional state and federal healthcare measures under the Trump administration will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand or lower pricing for our product candidates, or additional pricing pressures. Currently, the Health Care Reform Law provides coverage for smoking cessation-related activities, including two counseling attempts for smoking cessation per year and prescription drugs for smoking cessation, but not OTC treatments. If these provisions are repealed, in whole or in part, our business, financial condition or results of operations could be negatively affected.
Anti-Corruption. The Foreign Corrupt Practices Act of 1977, as amended, or FCPA, prohibits U.S. corporations and their representatives from offering, promising, authorizing or making payments to any foreign government official, government staff member, political party or political candidate in an attempt to obtain or retain business abroad. The scope of the FCPA includes interactions with certain healthcare professionals in many countries. Other countries have enacted similar anti-corruption laws and/or regulations. Individual states, acting through their attorneys general, have become active as well, seeking to regulate the marketing of prescription drugs under state consumer protection and false advertising laws.
Outside the United States
We expect to encounter similar regulatory and legislative issues in most other countries in which we seek to develop and commercialize cytisine.
New Drug Approvals and Pharmacovigilance. In the EU, the approval of new drugs may be achieved using the Mutual Recognition Procedure, the Decentralized Procedure or the EU Centralized Procedure. These procedures apply in the EU member states, plus the EEA countries, Norway, Iceland and Liechtenstein. The use of these procedures generally provides a more rapid and consistent approval process across the EU and EEA than was the case when the approval processes were operating independently within each country.
In 2012, new pharmacovigilance legislation came into force in the EU. Key changes include the establishment of a new Pharmacovigilance Risk Assessment Committee within the EMA, with responsibility for reviewing and making recommendations on product safety issues for the EU authorities. It also introduces the possibility for regulators to require pharmaceutical companies to conduct post-authorization efficacy studies at the time of approval, or at any time afterwards in light of scientific developments. There are also additional requirements regarding adverse drug reaction reporting and additional monitoring of products. Outside developed markets such as the EU and Japan, pharmacovigilance requirements vary and are typically less extensive.
The United Kingdom, or UK, is currently a member state of the EU. However, the UK has signaled its intention to withdraw from the EU, which is commonly known as BREXIT. Following BREXIT, if it occurs, the UK would no longer be a member state within the EU. Since a significant portion of the regulatory framework in the UK is derived from the regulations of the EU, BREXIT could materially change the regulatory framework applicable to the approval of our product candidates and other aspects of our business in the UK, such as the pricing and importation of prescription products. However, at this time it is not known what new regulatory
12
framework will be in place to govern the review and approval of new medicines in the UK. Further, the EMA is currently located in the UK. It is possible that BREXIT will result in a relocation of the EMA or disruption to the EMA’s review process.
Health authorities in many middle and lower income countries require marketing approval by a recognized regulatory authority (i.e., similar to the authority of the FDA or the EMA) before they begin to conduct their application review process and/or issue their final approval. Many authorities also require local clinical data in the country’s population in order to receive final marketing approval. These requirements delay marketing authorization in those countries relative to the United States and Europe.
CONTRACT RESEARCH AGREEMENTS
Our strategy is to outsource certain product development activities and have established contract research agreements for, preclinical, clinical, manufacturing and some data management services. We choose which business or institution to use for these services based on their expertise, capacity and reputation and the cost of the service.
We also provide or have provided quantities of our product candidates to academic research institutions to investigate the mechanism of action and evaluate novel combinations of product candidates with other cancer therapies in various cancer indications. These collaborations expand our research activities for our product candidates with modest contribution from us.
RESEARCH AND DEVELOPMENT EXPENDITURES
For the years ended December 31, 2017, 2016 and 2015, our expenditures for research and development activities were $3.1 million, $0.3 million and $0.1 million, respectively. Such research and development expenses primarily related to the advancement of our product candidate cytisine.
MANUFACTURING
We do not own or operate manufacturing facilities for the production of cytisine, nor do we have plans to develop our own manufacturing operations in the foreseeable future. We currently depend on Sopharma as supplier and contract manufacturer for all of our required raw materials, active pharmaceutical ingredients and finished product candidates for our clinical trials. Other than the Sopharma relationship, we do not have any current contractual arrangements for the manufacture of clinical or commercial supplies of cytisine. We currently employ internal resources and third-party consultants to manage our clinical manufacturing activities.
Sopharma sources cytisine from the Laburnum anagyroides plant, a shrub or small tree native to, and widely distributed throughout, Bulgaria, south Central Europe and the northwestern Balkan Peninsula. The seed pods are harvested from the shrubs and dried. Sopharma currently has planted approximately 225 acres of Laburnum trees, saplings and seedlings in multiple locations in Central and Eastern Bulgaria and is in the process of planting another 150 acres. Sopharma plans to plant additional trees to manage supply for major markets. Each tree takes approximately four to five years to reach maturity for harvesting and has a productive life expectancy of 20 to 25 years. Seeds are harvested annually, dried and stored for processing into cytisine. Laburnum seeds in their natural state are highly toxic and the extraction process removes the toxins to produce highly purified cytisine. Sopharma is stockpiling Laburnum seeds to meet the projected demand from us upon commercial launch.
The active pharmaceutical ingredient, or API, manufacturing process utilizes a series of techniques including milling, solvent extraction, filtration and purification. Critical control steps and manufacturing intermediates have been identified and are controlled by internally developed specifications and methods to ensure a consistent and reproducible process. The highly purified cytisine is dried, sieved and packed for storage until further processing into drug product. The cytisine API manufacturing process has been developed and refined over many years of manufacture by Sopharma, which has significant expertise in manufacturing cytisine.
Sopharma manufactures cytisine API in its facilities in Bulgaria, which are near the capital, Sofia. The API processing facility complies with EU cGMP requirements and has been inspected by the Bulgarian Drug Agency.
SALES AND MARKETING
Our commercial strategy may include the use of strategic partners, distributors, a contract sale force or the establishment of our own commercial and specialty sales force. We plan to further evaluate these alternatives. We intend to seek partners in territories where we have no commercial experience and intend to directly market in niche markets where a small cost-effective commercial capability can generate direct revenues.
13
The U.S. Supreme Court has held that certain claims to naturally-occurring substances are not patentable. Cytisine is a naturally-occurring product and is therefore not patentable in the United States. Furthermore, cytisine has been in use in other parts of the world for decades, and is not susceptible to patenting in its current form.
Our development and commercialization of cytisine is protected by our exclusive supply agreement with Sopharma and Sopharma’s proprietary technology, experience and expertise in cytisine extraction. In addition, we intend to utilize market exclusivity laws including those under the Hatch-Waxman Act in the United States and exclusivity under Directive 2004/27/EC in the EU.
Additionally, we are actively building an intellectual property portfolio around our clinical-stage product candidate and research programs. A key component of this portfolio strategy is to seek international patent protection with patent applications in the UK and in major market countries that we consider important to the development of our business worldwide. As of December 31, 2017, we had a portfolio of two international PCT applications of six priority patent applications pending in the UK. This portfolio includes method of use, formulation and composition of matter patents on cytisine and derivatives thereof.
We intend to make further international patent submissions, including in the United States, all of which will take patent filing priority dates from the UK applications referred to above. Our success depends in part on our ability to obtain and maintain proprietary protection for our product candidates and other discoveries, inventions, trade secrets and know-how that are critical to our business operations. Our success also depends in part on our ability to operate without infringing the proprietary rights of others, and in part, on our ability to prevent others from infringing our proprietary rights. A comprehensive discussion on risks relating to intellectual property is provided under “Risk Factors—Risks Related to Our Intellectual Property.”
In addition to patent protection, we rely on trade secrets, trademark protection and know-how to expand our proprietary position around our chemistry, technology and other discoveries and inventions that we consider important to our business. We also seek to protect our intellectual property in part by entering into confidentiality agreements with our employees, consultants, scientific advisors, clinical investigators and other contractors and also by requiring our employees, commercial contractors and certain consultants and investigators, to enter into invention assignment agreements that grant us ownership of any discoveries or inventions made by them.
COMPETITION
The development and commercialization of new products is highly competitive. We face competition from major pharmaceutical companies, specialty pharmaceutical companies, biotechnology companies, universities and other research institutions worldwide with respect to smoking cessation and other product candidates that it may seek to develop or commercialize in the future. We are aware that many companies have therapeutics marketed or in development for smoking cessation, including, Pfizer, GlaxoSmithKline, Merck, Novartis, Invion, Embera Neurotherapeutics, Redwood Scientific Technologies, 22nd Century Group, Quit4Good, Chrono Therapeutics, NAL Pharmaceuticals, Selecta Biosciences, Aradigm and others. We expect that our competitors and potential competitors have historically dedicated, and will continue to dedicate, significant resources to aggressively develop and commercialize their products in order to take advantage of the significant market opportunity.
Prescription Treatments
To our knowledge, two oral prescription drugs for smoking cessation are currently available in the United States – Chantix and Zyban. Both have been proven effective in aiding smoking cessation, however, each is associated with a number of adverse effects.
We believe that cytisine may have similar efficacy to Chantix with potential fewer adverse events and could be more cost-effective to patients. A Cochrane Group independent database review of nicotine receptor partial agonists published in 2016, or the Cochrane Report, compared cytisine with Chantix and found no apparent difference in efficacy between cytisine and Chantix, in that the database review found that the risk ratio for cytisine and Chantix was in the same order of magnitude. In addition, it should be noted that only two studies were used to calculate the risk ratio for cytisine versus 27 trials for varenicline, and that evidence for varenicline was considered of high and moderate quality while the evidence for cytisine was considered low quality. However, a head-to-head comparative trial of these two treatments has not been performed. Furthermore, a report by the National Institute of Health Research in the United Kingdom comparing Chantix and cytisine concluded that cytisine appears to be more clinically effective and cost effective than varenicline (Chantix) based on expected costs and quality-adjusted life-year, or QALY, values.
The Cochrane Report researchers searched for randomized controlled trials testing varenicline, cytisine or dianicline, finding 39 studies of varenicline compared to placebo, bupropion or nicotine patches. The Cochrane Report researchers also found four trials of cytisine, one of which compared it to nicotine replacement therapy. The Cochrane Report also included one trial of dianicline, which is no longer in development, and so not available to use as a smoking cessation aid. To be included, trials had to report quit rates at
14
least six months from the start of treatment. The Cochrane Report preferred the strictest available definition of quitting, and focused on results which had been biochemically confirmed by testing blood or bodily fluids. The Cochrane Report researchers conducted full searches up to May 2015, although several key trials published after that date were also included. The first cytisine trial included in the Cochrane Report was conducted in 1971. Since there are only two phase 3 studies with cytisine, the researchers that conducted the meta analysis included in the Cochrane report determined that their meta analysis was of poor quality.
Over-the-Counter Treatments
The most common OTC treatments bought in pharmacies for smoking cessation in the United States and worldwide are NRTs such as nicotine patches, nicotine gums and nicotine lozenges. Each of these products delivers nicotine to the body although they generally do so at different rates and to different parts of the body than does a traditional cigarette. As concluded by the authors of several published clinical trials conducted by others, these therapies are generally less effective than prescription treatments. Recognized brands include Niquitin ® , Nicotinell ® , Nicorette ® and Nicoderm ® . Depending on the duration of treatment, the average cost of certain OTC smoking cessation treatments can exceed prescription treatments.
Pharmaceutical companies, including larger companies in the industry, who have extensive expertise in pre-clinical and clinical testing and in obtaining regulatory approvals for products, may develop other OTC treatments for smoking cessation. In addition, academic institutions, government agencies and other public and private organizations conducting research may seek patent protection with respect to potentially competitive products or technologies. These organizations may also establish exclusive collaborative or licensing relationships with our competitors.
EMPLOYEES
As of December 31, 2017, we had a total of 13 employees, of whom five were engaged in research and development functions, including clinical development, regulatory affairs and manufacturing, and eight were engaged in general and administrative functions, including accounting and finance, administration, and corporate communications.
All of our employees have entered into non-disclosure agreements regarding our intellectual property, trade secrets and other confidential information. None of our employees are represented by a labor union or covered by a collective bargaining agreement, nor have we experienced any work stoppages. We believe that we maintain satisfactory relations with our employees.
From time to time, we also use outside consultants to provide advice on our clinical development plans, research programs, administration and potential acquisitions of new technologies.
FINANCIAL INFORMATION
We manage our operations and allocate resources as a single reporting segment. Financial information regarding our operations, assets and liabilities, including our total revenue and net loss for the years ended December 31, 2017, 2016 and 2015 and our total assets as of December 31, 2017 and 2016, is included in our Consolidated Financial Statements in Part II, Item 8 of this Annual Report on Form 10-K.
COMPANY INFORMATION
We were incorporated in California in October 1991 and subsequently reorganized as a Delaware corporation in March 1995. Our principal executive offices are located at 400 – 1001 W. Broadway Vancouver, B.C. V6H 4B1, and our telephone number is (604) 736-3678.
In August 2017, our company, then named OncoGenex Pharmaceuticals, Inc., completed its merger, or the Arrangement, with Achieve, as contemplated by the Merger Agreement between the companies. We then changed our name to Achieve Life Sciences, Inc. As a result of the Arrangement, Achieve became our wholly owned subsidiary. Achieve was formed in 2015 as a Delaware corporation and has one direct wholly-owned subsidiary, Extab Corporation, a Delaware corporation, which was formed in 2009. Extab Corporation in turn has one direct wholly-owned subsidiary, Achieve Pharma UK Limited, a United Kingdom company, which was formed in 2009. As used in this Annual Report on Form 10-K, the term “OncoGenex” refers to our business prior to August 1, 2017.
AVAILABLE INFORMATION
We maintain a website at http://www.achievelifesciences.com. The information contained on or accessible through our website is not part of this Annual Report on Form 10-K. Our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on
15
Form 8-K and amendments to reports filed or furnished pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended, or Exchange Act, are available free of charge on our website as soon as reasonably practicable after we electronically file such reports with, or furnish those reports to, the SEC. Any information we filed with the SEC may be accessed and copied at the SEC’s Public Reference Room at 100 F Street NE, Washington, DC 20549. Information may be obtained by calling the SEC at 1-800-SEC-0330. The SEC also maintains an Internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC at http://www.sec.gov.
Investing in our common stock involves a high degree of risk. You should consider carefully the risks and uncertainties described below, together with all of the other information contained in this Annual Report on Form 10-K and in the other periodic and current reports and other documents we file with the Securities and Exchange Commission, before deciding to invest in our common stock. If any of the following risks materialize, our business, financial condition, results of operation and future prospects will likely be materially and adversely affected. In that event, the market price of our common stock could decline and you could lose all or part of your investment. This list is not exhaustive and the order of presentation does not reflect management's determination of priority or likelihood.
Risks Related to Our Financial Condition and Capital Requirements
We have incurred losses since inception, have a limited operating history on which to assess our business and anticipate that we will continue to incur losses for the foreseeable future. We have never had any products available for commercial sale and we may never achieve or sustain profitability.
We are a clinical development-stage specialty pharmaceutical company with a limited operating history, are not profitable, have incurred losses in each year since our inception and do not expect to become profitable in the foreseeable future. We have never had any products available for commercial sale, and we have not generated any revenue from product sales, nor do we anticipate that we will generate revenue from product sales in the near future.
Pharmaceutical product development is a highly speculative undertaking and involves a substantial degree of risk. We have devoted substantially all of our financial resources to identify, acquire, and develop cytisine, including providing general and administrative support for our operations. To date, we have financed our operations primarily through the sale of equity securities and convertible promissory notes. The amount of our future net losses will depend, in part, on the rate of our future expenditures and our ability to obtain funding through equity or debt financings, strategic collaborations, or grants.
We expect to continue to incur significant expenses and increasing operating losses for the foreseeable future. We further expect that our expenses will increase substantially if and as we:
|
|
• |
continue the clinical development of cytisine; |
|
|
• |
advance cytisine development into larger, more expensive clinical trials; |
|
|
• |
initiate additional pre-clinical, clinical, or other trials or studies for cytisine; |
|
|
• |
seek to attract and retain skilled personnel; |
|
|
• |
undertake the manufacturing of cytisine or increase volumes manufactured by third parties; |
|
|
• |
seek regulatory and marketing approvals and reimbursement for cytisine; |
|
|
• |
make milestone, royalty or other payments under third-party license and/or supply agreements; |
|
|
• |
establish a sales, marketing, and distribution infrastructure to commercialize any product for which we may obtain marketing approval and market for ourselves; |
|
|
• |
continue efforts to discover new product candidates; |
|
|
• |
seek to identify, assess, acquire, and/or develop other product candidates; |
|
|
• |
seek to establish, maintain, protect, and expand our intellectual property portfolio; and |
|
|
• |
experience any delays or encounter issues with the development and potential for regulatory approval of cytisine such as safety issues, clinical trial accrual delays, longer follow-up for planned studies, additional major studies, or supportive studies necessary to support marketing approval. |
16
Further, the net losses we incur may fluctuate significantly from quarter to quarter and year to year, such that a period-to-period comparison of our results of operations may not be a good indication of our future performance.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our success at raising additional capital sufficient to meet our obligations on a timely basis. If we fail to obtain additional financing when needed, we may be unable to complete the development, regulatory approval and commercialization of our product candidates.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our ability to obtain additional financing. We have expended and continue to expend substantial funds in connection with our product development activities and clinical trials and regulatory approvals. In addition, we expect to incur significant expenses and increasing operating losses for at least the next several years as we continue our clinical development of, and seek regulatory approval for, cytisine and add personnel necessary to operate as a public company with an advanced clinical candidate. We expect that our operating losses will fluctuate significantly from quarter to quarter and year to year due to timing of clinical development programs and efforts to achieve regulatory approval.
Our current capital resources are insufficient to fund our planned operations for the next 12 months. We will continue to require substantial additional capital to continue our clinical development activities. Accordingly, we will need to raise substantial additional capital to continue to fund our operations from the sale of our securities, partnering arrangements or other financing transactions in order to finance the commercialization of our product candidates. The current financing environment in the United States, particularly for biotechnology companies like us, is exceptionally challenging and we can provide no assurances as to when such environment will improve. For these reasons, among others, we cannot be certain that additional financing will be available when and as needed or, if available, that it will be available on acceptable terms. If financing is available, it may be on terms that adversely affect the interests of our existing stockholders. If adequate financing is not available, we may need to continue to reduce or eliminate our expenditures for research and development of cytisine, and may be required to suspend development of cytisine. Our actual capital requirements will depend on numerous factors, including:
|
|
• |
our commercialization activities and arrangements; |
|
|
• |
the progress and results of our research and development programs; |
|
|
• |
the progress of our pre-clinical and clinical testing; |
|
|
• |
the time and cost involved in obtaining regulatory approvals for our product candidates; |
|
|
• |
the cost of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights with respect to our intellectual property; |
|
|
• |
the effect of competing technological and market developments; |
|
|
• |
the effect of changes and developments in our existing collaborative, licensing and other relationships; and |
|
|
• |
the terms of any new collaborative, licensing and other arrangements that we may establish. |
We may not be able to secure sufficient financing on acceptable terms, or at all. Without additional funds, we may be forced to delay, scale back or eliminate some of our research and development activities or other operations and potentially delay product development in an effort to provide sufficient funds to continue our operations. If any of these events occur, our ability to achieve our development and commercialization goals would be adversely affected.
We have never generated any revenue from product sales and may never be profitable.
We have no products approved for commercialization and have never generated any revenue from product sales. Our ability to generate revenue and achieve profitability depends on our ability, alone or with strategic collaborators, to successfully complete the development of, and obtain the regulatory and marketing approvals necessary to commercialize cytisine. We do not anticipate generating revenue from product sales for the foreseeable future. Our ability to generate future revenue from product sales depends heavily on our success in many areas, including but not limited to:
|
|
• |
completing research and development of cytisine; |
|
|
• |
obtaining regulatory and marketing approvals for cytisine; |
|
|
• |
manufacturing product and establishing and maintaining supply and manufacturing relationships with third parties that are commercially feasible, satisfy regulatory requirements and meet our supply needs in sufficient quantities to satisfy market demand for cytisine, if approved; |
17
|
|
• |
marketing, launching and commercializing any product for which we obtain regulatory and marketing approval, either directly or with a collaborator or distributor; |
|
|
• |
obtaining reimbursement or pricing for cytisine that supports profitability; |
|
|
• |
gaining market acceptance of cytisine as a treatment option; |
|
|
• |
addressing any competing products including the potential for generic cytisine products; |
|
|
• |
protecting and enforcing our intellectual property rights, if any, including patents, trade secrets, and know-how; |
|
|
• |
negotiating favorable terms in any collaboration, licensing, or other arrangements into which we may enter; and |
|
|
• |
attracting, hiring, and retaining qualified personnel. |
Even if a product candidate that we develop is approved for commercial sale, we anticipate incurring significant costs associated with commercializing that candidate. Additionally, if we are not able to generate sufficient revenue from the sale of any approved products to cover our operating costs, we may never become profitable. If we obtain regulatory approval to market a product candidate, our future revenue will depend upon the size of any markets in which our product candidates may receive approval, and our ability to achieve sufficient market acceptance, pricing, reimbursement from third-party payors, and adequate market share for our product candidates in those markets
We are dependent upon a single company for the manufacture and supply of cytisine.
Our single product candidate, cytisine, has been in-licensed from a third party. We are required to continue to contract with Sopharma AD, or Sopharma, to continue our development and commercialization, if any, of cytisine pursuant to a supply agreement with Sopharma. If the supply agreement with Sopharma is terminated, we will need to develop or acquire alternative supply and manufacturing capabilities for cytisine, which we may not be able to do on commercially viable terms or at all.
If we are unable to successfully commercialize cytisine due to failure to obtain regulatory approval or due to other risk factors outlined herein, our business, financial condition, and results of operations will be materially harmed as cytisine is currently our sole product candidate.
We recently completed the merger with OncoGenex Pharmaceuticals, Inc. and the failure to integrate successfully the operations of the combined company could adversely affect our future results.
Our success will depend, in significant part, on our ability to realize the anticipated benefits from combining the operations of the combined Achieve-OncoGenex enterprise. The failure to integrate successfully and to manage successfully the challenges presented by the integration process may result in our failure to achieve some or all of the anticipated benefits of the merger. Potential difficulties that may be encountered in the integration process include the following:
|
|
• |
using our cash and assets efficiently to develop our business; |
|
|
• |
appropriately managing our liabilities; |
|
|
• |
potential unknown or currently unquantifiable liabilities associated with the merger and our operations; |
|
|
• |
operating as a public company under our combined management team, some members of which have limited public company experience; and |
|
|
• |
performance shortfalls as a result of the diversion of the management’s attention caused by integrating the companies’ operations. |
We will incur costs and demands upon management as a result of complying with the laws and regulations affecting public companies.
We incur significant legal, accounting and other expenses associated with public company reporting requirements. We also incur costs associated with corporate governance requirements, including requirements under the Sarbanes-Oxley Act, as well as rules implemented by the SEC and The NASDAQ Capital Market. These rules and regulations impose significant legal and financial compliance costs and make some activities more time-consuming and costly. For example, our management team consists of certain executive officers of Achieve prior to the merger, some of whom have not previously managed and operated a public company. These executive officers and other personnel will need to devote substantial time to gaining expertise regarding operations as a public company and compliance with applicable laws and regulations. In addition, it may be more difficult for us to attract and retain
18
qualified individuals to serve on our board of directors or as executive officers, which may adversely affect investor confidence in our post-merger company and could cause our business or stock price to suffer.
Recently enacted comprehensive tax reform bills could increase our tax burden and adversely affect our business and financial condition.
The U.S. government has recently enacted comprehensive tax legislation that includes significant changes to the taxation of business entities. These changes include, among others, (i) a permanent reduction to the corporate income tax rate, (ii) a partial limitation on the deductibility of business interest expense, (iii) a shift of the U.S. taxation of multinational corporations from a tax on worldwide income to a territorial system (along with certain rules designed to prevent erosion of the U.S. income tax base) and (iv) a one-time tax on accumulated offshore earnings held in cash and illiquid assets, with the latter taxed at a lower rate.
In addition, beginning in 2022, the newly enacted tax legislation will require research and experimental expenditures to be capitalized and amortized ratably over a five-year period. Any such expenditures attributable to research conducted outside the U.S. must be capitalized and amortized over a 15-year period.
Notwithstanding the reduction in the corporate income tax rate, the overall impact of this tax reform is uncertain, and our business and financial condition could be adversely affected. In addition, it is uncertain if and to what extent various states will conform to the newly enacted federal tax law
Our principal stockholders own a significant percentage of our stock and will be able to exert significant control over us on matters subject to stockholder approval.
Our principal stockholders and their affiliates currently beneficially own approximately 53.1% of our outstanding voting stock. Therefore, these stockholders have the ability, and may continue to have the ability, to influence us through this ownership position. These stockholders are able to determine some or all matters involving us that require stockholder approval. For example, these stockholders, acting together, are able to control elections of directors, amendments of organizational documents, or approval of any merger, sale of assets, or other major corporate transaction. This control may prevent or discourage unsolicited acquisition proposals or offers for our common stock.
Risks Related to the Development of Our Product Candidates
Cytisine is currently our sole product candidate and there is no guarantee that we will be able to successfully develop and commercialize cytisine.
We are currently dependent on the potential development of a single product candidate, cytisine. We are still developing our sole product candidate, and cytisine cannot be marketed or sold in the United States or in foreign markets until regulatory approval has been obtained from the U.S. Food and Drug Administration, or the FDA, or applicable foreign regulatory agencies. The process of obtaining regulatory approval is expensive and time consuming. The FDA and foreign regulatory authorities may never approve cytisine for sale and marketing, and even if cytisine is ultimately approved, regulatory approval may be delayed or limited in the United States or in other jurisdictions. Even if we are authorized to sell and market cytisine in one or more markets, there is no assurance that we will be able to successfully market cytisine or that cytisine will achieve market acceptance sufficient to generate profits. Failure to develop cytisine, to obtain regulatory approval for cytisine, to successfully market cytisine, or to generate profits from the sale of cytisine would have material adverse effects on our business, financial condition, and results of operations.
Results of earlier clinical trials of cytisine are not necessarily predictive of future results, and any advances of cytisine into clinical trials may not have favorable results or receive regulatory approval.
Even if our clinical trials are completed as planned, we cannot be certain that their results will be consistent with the results of the earlier clinical trials of cytisine. Positive results in pre-clinical testing and past clinical trials with respect to the safety and efficacy of cytisine do not ensure that results from subsequent clinical trials will also be positive, and we cannot be sure that the results of subsequent clinical trials will replicate the results of prior clinical trials and pre-clinical testing. This failure may cause us to abandon cytisine, which would negatively affect our ability to generate any product revenues.
19
Clinical trials are costly, time consuming and inherently risky, and we may fail to demonstrate safety and efficacy to the satisfaction of applicable regulatory authorities.
Clinical development is expensive, time consuming and involves significant risk. We cannot guarantee that any clinical trial will be conducted as planned or completed on schedule, if at all. A failure of one or more clinical trials can occur at any stage of development. Events that may prevent successful or timely completion of clinical development include, but are not limited to:
|
|
• |
inability to generate satisfactory pre-clinical, toxicology, or other in vivo or in vitro data or diagnostics to support the initiation or continuation of clinical trials; |
|
|
• |
delays in reaching agreement on acceptable terms with clinical research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and clinical trial sites; |
|
|
• |
delays in obtaining required institutional review board, or IRB, approval at each clinical trial site; |
|
|
• |
failure to permit the conduct of a clinical trial by regulatory authorities, after review of an investigational new drug or equivalent foreign application or amendment; |
|
|
• |
delays in recruiting qualified patients in its clinical trials; |
|
|
• |
failure by clinical sites, CROs or other third parties to adhere to clinical trial requirements; |
|
|
• |
failure by clinical sites, CROs or other third parties to perform in accordance with the good clinical practices requirements of the FDA or applicable foreign regulatory guidelines; |
|
|
• |
patients terminating enrollment in our clinical trials; |
|
|
• |
adverse events or tolerability issues significant enough for the FDA or other regulatory agencies to put any or all clinical trials on hold; |
|
|
• |
animal toxicology issues significant enough for the FDA or other regulatory agencies to disallow investigation in humans; |
|
|
• |
occurrence of adverse events associated with our product candidate; |
|
|
• |
changes in regulatory requirements and guidance that require amending or submitting new clinical protocols; |
|
|
• |
the cost of clinical trials of cytisine; |
|
|
• |
negative or inconclusive results from our clinical trials which may result in us deciding, or regulators requiring us, to conduct additional clinical trials or abandon development programs in other ongoing or planned indications for cytisine; and |
|
|
• |
delays in the time for manufacture of sufficient quantities of cytisine for use in clinical trials. |
Any inability to successfully complete clinical development and obtain regulatory approval for cytisine could result in additional costs to us or impair our ability to generate revenue. In addition, if we make manufacturing or formulation changes to cytisine, we may need to conduct additional pre-clinical trials or the results obtained from such new formulation may not be consistent with previous results obtained. Clinical trial delays could also shorten any periods during which our products have patent protection and may allow competitors to develop and bring products to market before we do, which could impair our ability to successfully commercialize cytisine and may harm our business and results of operations.
Cytisine may cause undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial viability of an approved label, or result in significant negative consequences following marketing approval, if any.
Undesirable side effects caused by cytisine could cause us or regulatory authorities to interrupt, delay, or terminate clinical trials or even if approved, result in a restrictive label or delay regulatory approval by the FDA or comparable foreign authorities.
Additionally, even if cytisine receives marketing approval, and we or others later identify undesirable side effects caused by cytisine, potentially significant negative consequences could result, including but not limited to:
|
|
• |
regulatory authorities may withdraw approvals of cytisine; |
|
|
• |
regulatory authorities may require additional warnings on the cytisine label; |
20
|
|
• |
we could be sued and held liable for harm caused to patients; and |
|
|
• |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of cytisine, even if approved, and could significantly harm our business, results of operations, and prospects.
Our product development program may not uncover all possible adverse events that patients who take cytisine or our other product candidates may experience. The number of subjects exposed to cytisine or our other product candidates and the average exposure time in the clinical development program may be inadequate to detect rare adverse events, or chance findings, that may only be detected once the product is administered to more patients and for greater periods of time.
Clinical trials by their nature utilize a sample of the potential patient population. However, we cannot be fully assured that rare and severe side effects of cytisine will be uncovered. Such rare and severe side effects may only be uncovered with a significantly larger number of patients exposed to cytisine. If such safety problems occur or are identified after cytisine reaches the market in the United States, or if such safety problems occur or are identified in foreign markets where cytisine is currently marketed, the FDA may require that we amend the labeling of cytisine or recall it, or may even withdraw approval for cytisine.
If the use or misuse of cytisine harms patients, or is perceived to harm patients even when such harm is unrelated to cytisine, our regulatory approvals, if any, could be revoked or otherwise negatively impacted and we could be subject to costly and damaging product liability claims. If we are unable to obtain adequate insurance or are required to pay for liabilities resulting from a claim excluded from, or beyond the limits of, our insurance coverage, a material liability claim could adversely affect our financial condition.
The use or misuse of cytisine in clinical trials and the sale of cytisine if marketing approval is obtained, exposes us to the risk of potential product liability claims. Product liability claims might be brought against us by consumers, healthcare providers, pharmaceutical companies or others selling or otherwise coming into contact with our product. There is a risk that cytisine may induce adverse events. If we cannot successfully defend against product liability claims, we could incur substantial liability and costs. During the course of treatment, patients may suffer adverse events for reasons that may be related to cytisine. Such events could subject us to costly litigation, require us to pay substantial amounts of money to injured patients, delay, negatively impact or end our opportunity to receive or maintain regulatory approval to market cytisine, if any, or require us to suspend or abandon our commercialization efforts. Even in a circumstance in which an adverse event is unrelated to cytisine, the investigation into the circumstance may be time-consuming or inconclusive. These investigations may delay our regulatory approval process or impact and limit the type of regulatory approvals cytisine receives or maintains. As a result of these factors, a product liability claim, even if successfully defended, could have a material adverse effect on our business, financial condition or results of operations.
If we obtain marketing approval for cytisine, we will need to expand our insurance coverage to include the sale of commercial products. There is no way to know if we will be able to continue to obtain product liability coverage and obtain expanded coverage if we require it, in sufficient amounts to protect us against losses due to liability, on acceptable terms, or at all. We may not have sufficient resources to pay for any liabilities resulting from a claim excluded from, or beyond the limits of, our insurance coverage. Where we have provided indemnities in favor of third parties under our agreements with them, there is also a risk that these third parties could incur liability and bring a claim under such indemnities. An individual may bring a product liability claim against us alleging that cytisine causes, or is claimed to have caused, an injury or is found to be unsuitable for consumer use. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability, and a breach of warranties. Claims could also be asserted under state consumer protection acts. Any product liability claim brought against us, with or without merit, could result in:
|
|
• |
withdrawal of clinical trial volunteers, investigators, patients or trial sites or limitations on approved indications; |
|
|
• |
the inability to commercialize, or if commercialized, decreased demand for, cytisine; |
|
|
• |
if commercialized, product recalls, withdrawals of labeling, marketing or promotional restrictions or the need for product modification; |
|
|
• |
initiation of investigations by regulators; |
|
|
• |
loss of revenues; |
21
|
|
• |
liabilities that substantially exceed our product liability insurance, which we would then be required to pay ourselves; |
|
|
• |
an increase in our product liability insurance rates or the inability to maintain insurance coverage in the future on acceptable terms, if at all; |
|
|
• |
the diversion of management’s attention from our business; and |
|
|
• |
damage to our reputation and the reputation of our products and our technology. |
Product liability claims may subject us to the foregoing and other risks, which could have a material adverse effect on our business, financial condition or results of operations.
The development of our product candidate is dependent upon securing sufficient quantities of cytisine from the Laburnum anagyroides plant, which plant grows in a limited number of locations outside of the United States.
The therapeutic component of our product candidate, cytisine, is derived from the seeds of the Laburnum anagyroides plant, which grows in the mountains of Southern Europe. We currently secure cytisine exclusively from Sopharma, a Bulgarian third-party supplier. Our current supply agreement with Sopharma expires on July 28, 2037, unless extended by mutual agreement of us and Sopharma. There can be no assurances that Laburnum anagyroides will continue to grow in sufficient quantities to meet commercial supply requirements or that the countries from which we can secure Laburnum anagyroides will continue to allow the exportation of cytisine. Sopharma currently has planted approximately 600,000 laburnum trees, saplings and seedlings in multiple locations in Central and Eastern Bulgaria. Each tree takes approximately four to five years to reach maturity for harvesting and has a productive life expectancy of 20 to 25 years. Although Sopharma has plans to plant significant numbers of additional trees, there is no guarantee that they will do so or that the trees will produce the anticipated yield of cytisine. In the event we are no longer able to obtain cytisine from Sopharma, or in sufficient quantities, we may not be able to produce our proposed products and our business will be adversely affected.
Our business may be negatively affected by weather conditions and the availability of natural resources, as well as by climate change.
In recent years, extreme weather events and changing weather patterns such as storms, flooding, drought, and temperature changes, appear to have become more common. The production of cytisine from the Laburnum anagyroides plant depends on the availability of natural resources, including sufficient rainfall. Our exclusive supplier of cytisine, Sopharma, could be adversely affected if it experiences a shortage of fresh water due to droughts or other weather conditions. As a result of such events, we could experience cytisine shortages from Sopharma, all of which could have a material adverse effect on our business, financial condition and results of operations.
In addition, the manufacturing and other operations of Sopharma are located near earthquake fault lines in Sofia, Bulgaria. In the event of a major earthquake, we could experience business interruptions from the disruption of our cytisine supplies, which could have a material adverse effect on our business, financial condition and results of operations.
We may conduct clinical trials internationally, which may trigger additional risks.
If we decide to conduct clinical trials in Europe or other countries outside of the United States, we will have additional regulatory requirements that we will have to meet in connection with our manufacturing, distribution, use of data and other matters. The failure of us to meet such regulatory requirements could delay our clinical trials, the approval, if any, of cytisine by the FDA, or the commercialization of cytisine, or result in higher costs or deprive us of potential product revenues.
We may use our financial and human resources to pursue a particular research program or product candidate and fail to capitalize on programs or product candidates that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and human resources, we may forego or delay pursuit of opportunities with some programs or product candidates or for other indications that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or more profitable market opportunities. Our spending on current and future research and development programs and future product candidates for specific indications may not yield any commercially viable products. We may also enter into additional strategic collaboration agreements to develop and commercialize some of our programs and potential product candidates in indications with potentially large commercial markets. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product
22
candidate through strategic collaborations, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such product candidate, or we may allocate internal resources to a product candidate in a therapeutic area in which it would have been more advantageous to enter into a partnering arrangement.
Risks Related to Regulatory Approval of Cytisine and Other Legal Compliance Matters
If we do not obtain the necessary regulatory approvals in the United States and/or other countries, we will not be able to sell cytisine.
We will need approval from the FDA, to commercialize cytisine in the United States and approvals from similar regulatory authorities in foreign jurisdictions to commercialize cytisine in those jurisdictions. In order to obtain FDA approval of cytisine, we must submit an NDA to the FDA, demonstrating that cytisine is safe, pure and potent, and effective for its intended use. This demonstration requires significant research including completion of clinical trials. Satisfaction of the FDA’s regulatory requirements typically takes many years, depending upon the type, complexity and novelty of the product candidate and requires substantial resources for research, development and testing. We cannot predict whether our clinical trials will demonstrate the safety and efficacy of cytisine or if the results of any clinical trials will be sufficient to advance to the next phase of development or for approval from the FDA. We also cannot predict whether our research and clinical approaches will result in data that the FDA considers safe and effective for the proposed indications of cytisine. The FDA has substantial discretion in the product approval process. The approval process may be delayed by changes in government regulation, future legislation or administrative action or changes in FDA policy that occur prior to or during our regulatory review. While we intend to begin a pivotal Phase 3 trial in the first half of 2018, the FDA may require us to conduct additional Phase 3 trials, including if it deems the earlier trials involving cytisine to be insufficient or not available to support a single additional Phase 3 trial. Even if we comply with all FDA requests, the FDA may ultimately reject one or more of our applications. We may never obtain regulatory approval for cytisine. Failure to obtain approval from the FDA or comparable regulatory authorities in foreign jurisdictions to commercialize cytisine will leave us without saleable products and therefore without any source of revenues. In addition, the FDA may require us to conduct additional clinical testing or to perform post-marketing studies, as a condition to granting marketing approval of a product or permit continued marketing, if previously approved. If conditional marketing approval is obtained, the results generated after approval could result in loss of marketing approval, changes in product labeling, and/or new or increased concerns about the side effects or efficacy of a product. The FDA has significant post-market authority, including the explicit authority to require post-market studies and clinical trials, labeling changes based on new safety information and compliance with FDA-approved risk evaluation and mitigation strategies. The FDA’s exercise of its authority has in some cases resulted, and in the future could result, in delays or increased costs during product development, clinical trials and regulatory review, increased costs to comply with additional post-approval regulatory requirements and potential restrictions on sales of approved products. In foreign jurisdictions, the regulatory approval processes generally include the same or similar risks as those associated with the FDA approval procedures described above. We cannot be certain that we will receive the approvals necessary to commercialize cytisine for sale either within or outside the United States.
Even if we obtain regulatory approval for cytisine, we will remain subject to ongoing regulatory requirements in connection with the sale and distribution of cytisine.
Even if cytisine is approved by the FDA or comparable foreign regulatory authorities, we will be subject to ongoing regulatory requirements with respect to manufacturing, labeling, packaging, storage, advertising, promotion, sampling, record-keeping, conduct of post-marketing clinical trials, and submission of safety, efficacy and other post-approval information, including both federal and state requirements in the United States and the requirements of comparable foreign regulatory authorities. Compliance with such regulatory requirements will likely be costly and the failure to comply would likely result in penalties, up to and including, the loss of such approvals from the FDA or comparable foreign regulatory authorities.
Manufacturers and manufacturers’ facilities are required to continuously comply with FDA and comparable foreign regulatory authority requirements, including ensuring that quality control and manufacturing procedures conform to current Good Manufacturing Practices, or cGMP, regulations and corresponding foreign regulatory manufacturing requirements. As such, we, Sopharma and other contract manufacturers, if any, will be subject to continual review and inspections to assess compliance with cGMP and adherence to commitments made in any NDA or marketing authorization application.
Ongoing post-approval monitoring and clinical trial obligations may be costly to us and the failure to meet such obligations may result in the withdrawal of such approvals.
Any regulatory approvals that we receive for cytisine, if any, may be subject to limitations on the approved indicated uses for which cytisine may be marketed or to the conditions of approval, or contain requirements for potentially costly post-marketing testing, including Phase 4 clinical trials, and surveillance to monitor the safety and efficacy of cytisine. We will be required to report adverse
23
reactions and production problems, if any, to the FDA and comparable foreign regulatory authorities. Any new legislation addressing product safety issues could result in delays in product development or commercialization, or increased costs to assure compliance. If our original marketing approval for cytisine was obtained through an accelerated approval pathway, we could be required to conduct a successful post-marketing clinical trial in order to confirm the clinical benefit for our products. An unsuccessful post-marketing clinical trial or failure to complete such a trial could result in the withdrawal of marketing approval.
If a regulatory agency discovers previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is manufactured, or disagrees with the promotion, marketing or labeling of a product, the regulatory agency may impose restrictions on that product or us, including requiring withdrawal of the product from the market. If we fail to comply with applicable regulatory requirements, a regulatory agency or enforcement authority may, among other things:
|
|
• |
issue warning letters; |
|
|
• |
impose civil or criminal penalties; |
|
|
• |
suspend or withdraw regulatory approval; |
|
|
• |
suspend any of our ongoing clinical trials; |
|
|
• |
refuse to approve pending applications or supplements to approved applications submitted by us; |
|
|
• |
impose restrictions on our operations, including closing our contract manufacturers’ facilities; or |
|
|
• |
require a product recall. |
Any government investigation of alleged violations of law would be expected to require us to expend significant time and resources in response and could generate adverse publicity. Any failure to comply with ongoing regulatory requirements may significantly and adversely affect our ability to develop and commercialize our products and the value of us and our operating results would be adversely affected.
We may be subject, directly or indirectly, to federal and state healthcare fraud and abuse laws, false claims laws, and health information privacy and security laws. If we are unable to comply, or have not fully complied, with such laws, we could face substantial penalties.
If we obtain FDA approval for cytisine and begin commercializing it in the United States, our operations may be subject to various federal and state fraud and abuse laws, including, without limitation, the federal Anti-Kickback Statute, the federal False Claims Act, and physician sunshine laws and regulations. These laws may impact, among other things, our proposed sales, marketing, and education programs. In addition, we may be subject to patient privacy regulation by both the federal government and the states in which we conduct our business. The laws that may affect our ability to operate include:
|
|
• |
the federal Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, to induce, or in return for, the purchase or recommendation of an item or service reimbursable under a federal healthcare program, such as the Medicare and Medicaid programs; |
|
|
• |
federal civil and criminal false claims laws and civil monetary penalty laws, which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent; |
|
|
• |
the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, which created new federal criminal statutes that prohibit executing a scheme to defraud any healthcare benefit program and making false statements relating to healthcare matters; |
|
|
• |
HIPAA, as amended by the Health Information Technology and Clinical Health Act, and its implementing regulations, which imposes specified requirements relating to the privacy, security, and transmission of individually identifiable health information; |
|
|
• |
HIPAA, as amended by the Health Information Technology and Clinical Health Act, and its implementing regulations, which imposes specified requirements relating to the privacy, security, and transmission of individually identifiable health information; |
24
|
|
devices, biologics, and medical supplies to report annually to the U.S. Department of Health and Human Services information related to payments and other transfers of value to physicians, other healthcare providers, and teaching hospitals, and ownership and investment interests held by physicians and other healthcare providers and their immediate family members and applicable group purchasing organizations; and |
|
|
• |
state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws that may apply to items or services reimbursed by any third-party payor, including governmental and private payors, to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws that require product manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures, and state laws governing the privacy and security of health information in specified circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts. |
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available, it is possible that some of our business activities could be subject to challenge under one or more of such laws. In addition, recent health care reform legislation has strengthened these laws. For example, the Health Care Reform Law, among other things, amends the intent requirement of the federal anti-kickback and criminal healthcare fraud statutes. A person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. Moreover, the Health Care Reform Law provides that the government may assert that a claim including items or services resulting from a violation of the federal anti-kickback statute constitutes a false or fraudulent claim for purposes of the False Claims Act.
If our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from participation in government health care programs, such as Medicare and Medicaid, imprisonment, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and its results of operations.
Healthcare legislative and executive reform measures may have a material adverse effect on our business, financial condition or results of operations.
In the United States, there have been and continue to be a number of legislative initiatives to contain healthcare costs. For example, in March 2010, the Health Care Reform Law was passed, which substantially changes the way health care is financed by both governmental and private insurers, and significantly impacts the U.S. pharmaceutical industry. The Health Care Reform Law, among other things, addresses a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for products that are inhaled, infused, instilled, implanted, or injected, increases the minimum Medicaid rebates owed by manufacturers under the Medicaid Drug Rebate Program and extends the rebate program to individuals enrolled in Medicaid managed care organizations, establishes annual fees and taxes on manufacturers of specified branded prescription products, and promotes a new Medicare Part D coverage gap discount program.
On January 20, 2017, President Donald Trump issued an Executive Order to initiate the repeal of the Health Care Reform Law and we expect that additional state and federal healthcare measures under the Trump administration will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand or lower pricing for cytisine, or additional pricing pressures. Currently, the Health Care Reform Law provides coverage for smoking cessation-related activities, including two counseling attempts for smoking cessation per year and prescription drugs for smoking cessation, but not over-the-counter treatments. If these provisions are repealed, in whole or in part, our business, financial condition, or results of operations could be negatively affected.
The United Kingdom is currently a member state of the European Union. However, the United Kingdom has signaled its intention to withdraw from the European Union (commonly known as BREXIT). If BREXIT, which is likely to occur in 2019, does occur, the United Kingdom will no longer be a member state within the European Union. Since a significant portion of the regulatory framework in the United Kingdom is derived from the regulations of the European Union, BREXIT could materially change the regulatory framework applicable to the approval of cytisine, which could have a material adverse effect on us and our operations. BREXIT may also result in other significant regulatory and legislative changes in the United Kingdom, which could, for example, affect the pricing of pharmaceutical products in the United Kingdom, which could in turn result in diminished performance for us. Even if the substance of regulatory changes resulting from BREXIT does not have a significant impact on our operations, it is reasonable to expect that we would incur potentially significant costs in connection with complying with any new regulations. Further, the European Medicines Agency is currently located in the United Kingdom. It is possible that BREXIT would result in the relocation of the European Medicines Agency or disruption to the European Medicines Agency’s review process, either of which could have an adverse effect on our operations in the United Kingdom and the European Union.
25
BREXIT may also have adverse effects on potential customers and collaborators of ours, which could indirectly have an adverse effect on us.
Risks Related to our Business Operations
It is difficult to evaluate our current business, predict our future prospects and forecast our financial performance and growth.
To date our business activities have been focused primarily on the development and regulatory approval of cytisine and its various alternative forms. Although we have not generated revenue to date, we expect that, after any regulatory approval, any receipt of revenue will be attributable to sales of cytisine, primarily in the United States, the European Union (including the United Kingdom) and Japan. Because we devote substantially all of our resources to the development of cytisine and rely on cytisine as our sole source of potential revenue for the foreseeable future, any factors that negatively impact this product, or result in decreasing product sales, would materially and adversely affect our business, financial condition and results of operations.
Our future success depends in part on our ability to attract, retain, and motivate other qualified personnel.
We will need to expand and effectively manage our managerial, operational, financial, development and other resources in order to successfully pursue our development and commercialization efforts for our existing and future product candidates. We expect to need additional scientific, technical, operational, financial and other personnel. Our success depends on our continued ability to attract, retain and motivate highly qualified personnel, such as management, clinical and preclinical personnel, including our executive officers Richard Stewart, John Bencich, Cindy Jacobs, Anthony Clarke and Jaime Welch. In addition, although we have entered into employment agreements with each of Mr. Stewart, Mr. Bencich, Dr. Jacobs, Dr. Clarke and Ms. Welch, such agreements permit those executives to terminate their employment with us at any time, subject to providing us with advance written notice
We may not be able to attract and retain personnel on acceptable terms, if at all, given the competition among numerous pharmaceutical and biotechnology companies for individuals with similar skill sets. In addition, failure to succeed in development and commercialization of cytisine may make it more challenging to recruit and retain qualified personnel. The inability to recruit and retain qualified personnel, or the loss of the services of our current personnel may impede the progress of our research, development, and commercialization objectives and would negatively impact our ability to succeed in our product development strategy.
We will need to expand our organization and we may experience difficulties in managing this growth, which could disrupt our operations.
We may need to divert a disproportionate amount of our attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. We may not be able to effectively manage the expansion of our operations, which may result in weaknesses in its infrastructure, operational mistakes, loss of business opportunities, loss of employees, and reduced productivity among remaining employees. Our expected growth could require significant capital expenditures and may divert financial resources from other projects, such as the development of additional product candidates. If we are unable to effectively manage our growth, our expenses may increase more than expected, our ability to generate and/or grow revenue could be reduced and we may not be able to implement our business strategy. Our future financial performance and our ability to commercialize product candidates and compete effectively will depend, in part, on our ability to effectively manage any future growth.
Risks Related to Our Reliance on Third Parties
We expect to continue to rely on third parties to manufacture cytisine for use in clinical trials, and we intend to exclusively rely on Sopharma to produce and process cytisine, if approved. Our commercialization of cytisine could be stopped, delayed or made less profitable if Sopharma fails to obtain approval of government regulators, fails to provide us with sufficient quantities of product, or fails to do so at acceptable quality levels or prices.
We do not currently have nor do we currently plan to develop the infrastructure or capability internally to manufacture our clinical supplies for use in the conduct of our clinical trials, and we lack the resources and the capability to manufacture cytisine on a clinical or commercial scale. We currently exclusively rely on Sopharma to manufacture cytisine for use in clinical trials and plan to continue relying on Sopharma to manufacture cytisine on a commercial scale, if approved.
Our reliance on Sopharma exposes us to the following additional risks:
|
|
• |
Sopharma might be unable to timely manufacture cytisine or produce the quantity and quality required to meet our clinical and commercial needs, if any; |
|
|
• |
we may be unable to identify manufacturers other than Sopharma on acceptable terms or at all; |
|
|
• |
Sopharma may not be able to execute our manufacturing procedures appropriately; |
26
|
|
• |
Sopharma may not perform as agreed or may not remain in the contract manufacturing business for the time required to supply our clinical trials or to successfully produce, store and distribute our products; |
|
|
• |
Sopharma is or will be subject to ongoing periodic unannounced inspection by the FDA and corresponding state agencies to ensure strict compliance with cGMPs and other government regulations and corresponding foreign standards. We do not have control over Sopharma’s compliance with these regulations and standards; |
|
|
• |
we may not own, or may have to share, the intellectual property rights to any improvements made by Sopharma in the manufacturing process for cytisine; |
|
|
• |
we do not own the intellectual property rights to cytisine, and Sopharma could license such rights to third parties or begin supplying other third parties with cytisine; and |
|
|
• |
Sopharma could breach or terminate their agreement with us. |
Each of these risks could delay our clinical trials, the approval, if any of cytisine by the FDA or the commercialization of cytisine or result in higher costs or deprive us of potential product revenue.
The manufacture of medical products is complex and requires significant expertise and capital investment, including the development of advanced manufacturing techniques and process controls. Manufacturers of medical products often encounter difficulties in production, particularly in scaling up and validating initial production and absence of contamination. These problems include difficulties with production costs and yields, quality control, including stability of the product, quality assurance testing, operator error, shortages of qualified personnel, as well as compliance with strictly enforced federal, state and foreign regulations. Furthermore, if contaminants are discovered in the supply of cytisine or in the Sopharma manufacturing facilities, such manufacturing facilities may need to be closed for an extended period of time to investigate and remedy the contamination. We cannot be assured that any stability or other issues relating to the manufacture of cytisine will not occur in the future. Additionally, Sopharma may experience manufacturing difficulties due to resource constraints or as a result of labor disputes or political instability in the countries in which Sopharma conducts its operations. If Sopharma were to encounter any of these difficulties, or otherwise fail to comply with its contractual obligations, our ability to provide our product candidates to patients in clinical trials could be delayed or suspended. Any delay or interruption in the supply of clinical trial supplies could delay the completion of clinical trials, increase the costs associated with maintaining clinical trial programs and, depending upon the period of delay, require us to commence new clinical trials at additional expense or terminate clinical trials completely. Similar political instability could also harm the commercial production and supply of cytisine in the event that cytisine is ultimately approved for commercial sale.
We rely on third parties to conduct our clinical trials and perform other services. If these third parties do not successfully perform and comply with regulatory requirements, we may not be able to successfully complete clinical development, obtain regulatory approval or commercialize cytisine and our business could be substantially harmed.
We plan to rely upon third-party CROs to conduct, monitor and manage our ongoing clinical programs. We rely on these parties for execution of clinical trials and manage and control only some aspects of their activities. We remain responsible for ensuring that each of our trials is conducted in accordance with the applicable protocol, legal, regulatory, and scientific standards and our reliance on the CROs does not relieve us of our regulatory responsibilities. We and our CROs and other vendors are required to comply with all applicable laws, regulations and guidelines, including those required by the FDA and comparable foreign regulatory authorities for all of our product candidates in clinical development. If we or any of our CROs or vendors fail to comply with applicable laws, regulations and guidelines, the results generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot be assured that our CROs and other vendors will meet these requirements, or that upon inspection by any regulatory authority, such regulatory authority will determine that efforts, including any of our clinical trials, comply with applicable requirements. Our failure to comply with these laws, regulations and guidelines may require us to repeat clinical trials, which would be costly and delay the regulatory approval process.
If any of our relationships with these third-party CROs terminate, we may not be able to enter into arrangements with alternative CROs in a timely manner or do so on commercially reasonable terms. In addition, our CROs may not prioritize our clinical trials relative to those of other customers and any turnover in personnel or delays in the allocation of CRO employees by the CRO may negatively affect our clinical trials. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, continued development of cytisine may be delayed or terminated and we may not be able to meet our current plans with respect to cytisine. CROs may also involve higher costs than anticipated, which could negatively affect our financial condition and operations.
27
We may not be able to establish or maintain the third-party relationships that are necessary to develop or potentially commercialize cytisine.
Our business plan relies heavily on third party collaborators, partners, licensees, clinical research organizations, clinical investigators, vendors or other third parties to support our research and development efforts and to conduct clinical trials for cytisine. We cannot guarantee that we will be able to successfully negotiate agreements for, or maintain relationships with, these third parties on a commercially reasonable basis, if at all. If we fail to establish or maintain such third-party relationships as anticipated, our business could be adversely affected.
We may be unable to realize the potential benefits of any collaborations which we may enter into with other companies for the development and commercialization of cytisine.
We may enter into a collaboration with third parties concerning the development and/or commercialization of cytisine; however, there is no guarantee that any such collaboration will be successful. Collaborations may pose a number of risks, including:
|
|
• |
collaborators often have significant discretion in determining the efforts and resources that they will apply to the collaboration, and may not commit sufficient resources to the development, marketing or commercialization of cytisine; |
|
|
• |
collaborators may not perform their obligations as expected; |
|
|
• |
any such collaboration may significantly limit our share of potential future profits from the associated program, and may require us to relinquish potentially valuable rights to cytisine, or other potential products or proprietary technologies or grant licenses on terms that are not favorable to us; |
|
|
• |
collaborators may cease to devote resources to the development or commercialization of cytisine if the collaborators view cytisine as competitive with their own products or product candidates; |
|
|
• |
disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the course of development, might cause delays or termination of the development or commercialization of cytisine, and might result in legal proceedings, which would be time consuming, distracting and expensive; |
|
|
• |
collaborators may be impacted by changes in their strategic focus or available funding, or business combinations involving them, which could cause them to divert resources away from the collaboration; |
|
|
• |
collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; |
|
|
• |
the collaborations may not result in us achieving revenues to justify such transactions; and |
|
|
• |
collaborations may be terminated and, if terminated, may result in a need for us to raise additional capital to pursue further development or commercialization of cytisine. |
As a result, a collaboration may not result in the successful development or commercialization of cytisine.
We enter into various contracts in the normal course of our business in which we indemnify the other party to the contract. In the event we have to perform under these indemnification provisions, it could have a material adverse effect on our business, financial condition and results of operations.
In the normal course of business, we enter into academic, commercial, service, collaboration, licensing, consulting and other agreements that contain indemnification provisions. With respect to our academic and other research agreements, we typically indemnify the institution and related parties from losses arising from claims relating to the products, processes or services made, used, sold or performed pursuant to the agreements for which we have secured licenses, and from claims arising from our or our sublicensees’ exercise of rights under the agreement. With respect to our collaboration agreements, we indemnify our collaborators from any third-party product liability claims that could result from the production, use or consumption of the product, as well as for alleged infringements of any patent or other intellectual property right by a third party. With respect to consultants, we indemnify them from claims arising from the good faith performance of their services.
Should our obligation under an indemnification provision exceed applicable insurance coverage or if we were denied insurance coverage, our business, financial condition and results of operations could be adversely affected. Similarly, if we are relying on a collaborator to indemnify us and the collaborator is denied insurance coverage or the indemnification obligation exceeds the applicable insurance coverage, and if the collaborator does not have other assets available to indemnify us, our business, financial condition and results of operations could be adversely affected.
28
Risks Related to Commercialization of Cytisine
We face substantial competition and our competitors may discover, develop or commercialize products faster or more successfully than us.
The development and commercialization of new products is highly competitive. We face competition from major pharmaceutical companies, specialty pharmaceutical companies, biotechnology companies, universities and other research institutions worldwide with respect to cytisine and the other product candidates that we may seek to develop or commercialize in the future. We are aware that many companies have therapeutics marketed or in development for smoking cessation, including, Pfizer Inc., GlaxoSmithKline Plc, Merck & Co., Novartis, Invion, Embera Neurotherapeutics, Redwood Scientific Technologies, Inc., 22nd Century Group, Inc., Quit4Good, Chrono Therapeutics, NAL Pharmaceuticals, Selecta Biosciences, Aradigm and others.
Many of our competitors have substantially greater financial, name recognition, manufacturing, marketing, research, technical and other resources than us. Additional mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated in our competitors. Further, our competitors may develop new products that are safer, more effective or more cost-efficient than cytisine. Large pharmaceutical companies in particular have extensive expertise in pre-clinical and clinical testing and in obtaining regulatory approvals for products. In addition, academic institutions, government agencies, and other public and private organizations conducting research may seek patent protection with respect to potentially competitive products or technologies. These organizations may also establish exclusive collaborative or licensing relationships with our competitors. Failure of cytisine to effectively compete against established treatment options or in the future with new products currently in development would harm our business, financial condition, results of operations and prospects.
The commercial success of cytisine will depend upon the degree of market acceptance by physicians, patients, third-party payors, and others in the medical community. Failure to obtain or maintain adequate reimbursement or insurance coverage for products, if any, could limit our ability to market cytisine and decrease our ability to generate revenue.
Even with the approvals from the FDA and comparable foreign regulatory authorities, the commercial success of cytisine will depend in part on the health care providers, patients, and third-party payors accepting cytisine as medically useful, cost-effective, and safe. Cytisine may not gain market acceptance by physicians, patients and third-party payors. The degree of market acceptance of cytisine will depend on a number of factors, including but not limited to:
|
|
• |
the efficacy, if any, of cytisine as demonstrated in clinical trials and potential advantages over competing treatments, if any; |
|
|
• |
the clinical indications for which approval is granted, if any, including any limitations or warnings contained in cytisine’s approved labeling; |
|
|
• |
the cost of treatment; |
|
|
• |
the perceived ratio of risk and benefit of these therapies by physicians and the willingness of physicians to recommend the product to patients based on such risks and benefits; |
|
|
• |
the marketing, sales and distribution support for cytisine; |
|
|
• |
the publicity concerning cytisine or competing products and treatments; |
|
|
• |
the pricing and availability of third-party insurance coverage and reimbursement; and |
|
|
• |
negative perceptions or experiences with our competitor’s products may be ascribed to cytisine. |
Even if cytisine displays a favorable efficacy and safety profile upon approval, market acceptance of cytisine remains uncertain. Efforts to educate the medical community and third-party payors on the benefits of cytisine, if any, may require significant investment and resources and may never be successful. Additionally, third-party payors, including governmental and private insurers, may also encourage the use of generic products instead of cytisine, which require a prescription. If our products fail to achieve an adequate level of acceptance by physicians, patients, third-party payors, and other health care providers, we will not be able to generate sufficient revenue to become or remain profitable.
The pricing, coverage, and reimbursement of cytisine, if any, must be sufficient to support our commercial efforts and other development programs and the availability and adequacy of coverage and reimbursement by third-party payors, including governmental and private insurers, are essential for most patients to be able to afford treatments. Sales of cytisine, if any, will depend substantially, both domestically and abroad, on the extent to which the costs of cytisine will be paid for or reimbursed by health maintenance, managed care, pharmacy benefit and similar healthcare management organizations, or government payors and private
29
payors. If coverage and reimbursement are not available, or are available only in limited amounts, we may have to subsidize or provide cytisine for free or we may not be able to successfully commercialize cytisine.
In addition, there is significant uncertainty related to the insurance coverage and reimbursement for newly approved products. In the United States, the principal decisions about coverage and reimbursement for new products are typically made by the Centers for Medicare and Medicaid Services, or CMS, an agency within the U.S. Department of Health and Human Services, as CMS decides whether and to what extent a new product will be covered and reimbursed under Medicare. Private payors tend to follow the coverage reimbursement policies established by CMS to a substantial degree. It is difficult to predict what CMS will decide with respect to reimbursement for novel product candidates such as cytisine and what reimbursement codes cytisine may receive if approved.
Outside the United States, selling operations are generally subject to extensive governmental price controls and other price-restrictive regulations, and we believe the increasing emphasis on cost-containment initiatives in Europe, Canada, and other countries has and will continue to put pressure on the pricing and usage of products. In many countries, the prices of products are subject to varying price control mechanisms as part of national health systems. Price controls or other changes in pricing regulation could restrict the amount that we are able to charge for our products, if any. Accordingly, in markets outside the United States, the potential revenue may be insufficient to generate commercially reasonable revenue and profits.
Moreover, increasing efforts by governmental and private payors in the United States and abroad to limit or reduce healthcare costs may result in restrictions on coverage and the level of reimbursement for new products and, as a result, they may not cover or provide adequate payment for our products. We expect to experience pricing pressures in connection with products due to the increasing trend toward managed healthcare, including the increasing influence of health maintenance organizations and additional legislative changes. The downward pressure on healthcare costs in general, particularly prescription products has and is expected to continue to increase in the future. As a result, profitability of cytisine, if any, may be more difficult to achieve even if regulatory approval is received.
Sopharma may breach its supply agreement with us and sell cytisine into our territories or permit third parties to export cytisine into our territories and negatively affect our commercialization efforts of our products in our territories.
We are currently dependent on the exclusivity provisions of our supply agreement with Sopharma to conduct our business and to prevent Sopharma from competing, directly and indirectly, with us in the United States and Western Europe. If Sopharma were to breach the exclusivity provisions of the supply agreement with us and sell or distribute cytisine directly into our territories or permit third parties to export cytisine into our territories, among other things, the increase in competition within our anticipated markets could have a material adverse effect on our business, results of operations and financial condition.
The illegal distribution and sale by third parties of counterfeit versions of cytisine, stolen products, or alternative third party distribution and sale of cytisine could have a negative impact on our financial performance or reputation.
Cytisine is not patentable in the United States as it is a naturally occurring substance. As such, third parties are able to manufacture, sell or distribute cytisine without royalties or other payments to us and compete with our products in the United States and potentially worldwide and negatively impact our commercialization efforts of our products. Other than regulatory exclusivity or other limitations, there may be little to nothing to stop these third parties from manufacturing, selling or distributing cytisine. Because we have no ability to set rigorous safety standards or control processes over third party manufacturers, sellers or distributors of cytisine, excluding Sopharma, these formulations of cytisine may be unsafe or cause adverse effects to patients and negatively impact the reputation of cytisine as a safe and effective smoking cessation aid.
Third parties could illegally distribute and sell counterfeit versions of cytisine, especially on online marketplaces, which do not meet the rigorous manufacturing and testing standards under cGMP. Counterfeit products are frequently unsafe or ineffective, and may even be life-threatening. Counterfeit medicines may contain harmful substances, the wrong dose of the active pharmaceutical ingredient or no active pharmaceutical ingredients at all. However, to distributors and users, counterfeit products may be visually indistinguishable from the authentic version.
Reports of adverse reactions to counterfeit products, increased levels of counterfeiting, or unsafe cytisine products could materially affect patient confidence in our cytisine product. It is possible that adverse events caused by unsafe counterfeit or other non-Achieve cytisine products will mistakenly be attributed to our cytisine product. In addition, thefts of inventory at warehouses, plants or while in-transit, which are not properly stored and which are sold through unauthorized channels could adversely impact patient safety, our reputation, and our business. Public loss of confidence in the integrity in cytisine as a result of counterfeiting, theft, or improper manufacturing processes could have a material adverse effect on our business, results of operations, and financial condition.
It is illegal to sell unapproved prescription medicines in the United States. Sopharma’s cytisine brand, Tabex, is currently approved for sale in certain Central and Eastern European countries. Cytisine has not yet received a marketing approval from the FDA or the
30
European Medicines Agency, and we intend to conduct the requisite clinical trials to obtain approval for the marketing of cytisine in the United States and in Europe. We are aware that products purporting to be Tabex are available, via third party internet sites, for importation in the United States and European Union. We have no control over the authenticity of products purchased through these sites, which may be counterfeit or sourced from distributors in Central and Eastern Europe without authorization to sell into the United States or European Union.
We may attempt to form collaborations in the future with respect to cytisine, but we may not be able to do so, which may cause us to alter our development and commercialization plans.
We may attempt to form strategic collaborations, create joint ventures or enter into licensing arrangements with third parties with respect to our programs that we believe will complement or augment our existing business. We may face significant competition in seeking appropriate strategic collaborators, and the negotiation process to secure appropriate terms is time consuming and complex. We may not be successful in our efforts to establish such a strategic collaboration for cytisine on terms that are acceptable to us, or at all. This may be because cytisine may be deemed to be at too early of a stage of development for collaborative effort, our research and development pipeline may be viewed as insufficient, the competitive or intellectual property landscape may be viewed as too intense or risky, or cytisine’s patent protection insufficient, and/or third parties may not view cytisine as having sufficient potential for commercialization, including the likelihood of an adequate safety and efficacy profile.
Any delays in identifying suitable collaborators and entering into agreements to develop and/or commercialize cytisine could delay the development or commercialization of cytisine, which may reduce our competitiveness even if we reach the market. Absent a strategic collaborator, we would need to undertake development and/or commercialization activities at our own expense. If we elect to fund and undertake development and/or commercialization activities on our own, we may need to obtain additional expertise and additional capital, which may not be available to us on acceptable terms or at all. If we are unable to do so, we may not be able to develop our product candidates or bring them to market and our business may be materially and adversely affected.
We may not be successful in any efforts to identify, license, discover, develop, or commercialize additional product candidates.
Although a substantial amount of our effort will focus on clinical testing, approval, and potential commercialization of cytisine, our sole product candidate, the success of our business is also expected to depend in part upon our ability to identify, license, discover, develop, or commercialize additional product candidates. Research programs to identify new product candidates require substantial technical, financial, and human resources. We may focus our efforts and resources on potential programs or product candidates that ultimately prove to be unsuccessful. Our research programs or licensing efforts may fail to yield additional product candidates for clinical development and commercialization for a number of reasons, including but not limited to the following:
|
|
• |
Our research or business development methodology or search criteria and process may be unsuccessful in identifying potential product candidates; |
|
|
• |
we may not be able or willing to assemble sufficient resources to acquire or discover additional product candidates; |
|
|
• |
our product candidates may not succeed in pre-clinical or clinical testing; |
|
|
• |
our potential product candidates may be shown to have harmful side effects or may have other characteristics that may make the products unmarketable or unlikely to receive marketing approval; |
|
|
• |
competitors may develop alternatives that render our product candidates obsolete or less attractive; |
|
|
• |
product candidates we develop may be covered by third parties’ patents or other exclusive rights; |
|
|
• |
the market for a product candidate may change during our program so that such a product may become unreasonable to continue to develop; |
|
|
• |
a product candidate may not be capable of being produced in commercial quantities at an acceptable cost, or at all; and |
|
|
• |
a product candidate may not be accepted as safe and effective by patients, the medical community, or third-party payors. |
If any of these events occur, we may be forced to abandon our development efforts for a program or programs, or we may not be able to identify, license, discover, develop, or commercialize additional product candidates, which would have a material adverse effect on our business, financial condition or results of operations and could potentially cause us to cease operations.
31
Risks Related to our Intellectual Property
We may not be successful in obtaining or maintaining necessary rights to cytisine, product compounds and processes for our development pipeline through acquisitions and in-licenses.
Presently, we have rights to the intellectual property through trade secrets, licenses from third parties and patent applications that we own. Our product candidates may require specific formulations to work effectively and efficiently and these rights may be held by others. We may be unable to acquire or in-license any compositions, methods of use, processes or other third-party intellectual property rights from third parties that we identify. The licensing and acquisition of third-party intellectual property rights is a competitive area, and a number of more established companies are also pursuing strategies to license or acquire third-party intellectual property rights that we may consider attractive. These established companies may have a competitive advantage over us due to their size, cash resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment. If we are unable to successfully obtain rights to third-party intellectual property rights, our business, financial condition and prospects for growth could suffer.
If we are unable to maintain effective proprietary rights for our product candidates or any future product candidates, we may not be able to compete effectively in our proposed markets.
We currently rely primarily on trade secret protection and on confidentiality agreements to protect proprietary know-how that is not patentable or that we elect not to patent, processes for which patents are difficult to enforce and any other elements of our product candidate discovery and development processes that involve proprietary know-how, information or technology that is not covered by patents. Trade secrets can be difficult to protect, however, and even where they are protected they generally provide less intellectual property protection to the holder of the trade secret than to a holder of a patent. We seek to protect our proprietary technology and processes, in part, by entering into confidentiality agreements with our employees, consultants, scientific advisors, and contractors. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, agreements or security measures may be breached, and we may not have adequate remedies for any breach. In addition, our trade secrets may otherwise become known or be independently discovered by competitors.
Although we expect all of our employees and consultants to assign their inventions to us, and all of our employees, consultants, advisors, and any third parties who have access to our proprietary know-how, information, or technology to enter into confidentiality agreements, we cannot provide any assurances that all such agreements have been duly executed or that our trade secrets and other confidential proprietary information will not be disclosed or that competitors will not otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. Misappropriation or unauthorized disclosure of our trade secrets could impair our competitive position and may have a material adverse effect on our business, financial condition or results of operations. Additionally, if the steps taken to maintain our trade secrets are deemed inadequate, we may have insufficient recourse against third parties for misappropriating the trade secret.
Third-party claims of intellectual property infringement may prevent or delay our development and commercialization efforts.
We are currently developing cytisine for smoking cessation. Our commercial success depends in part on our ability to develop, manufacture, market and sell our product candidates and use our proprietary technology without infringing the patent rights of third parties. We are not aware of any patents or patent applications that would prevent the development, manufacture or marketing of cytisine for smoking cessation.
We are aware of U.S. and foreign patents and pending patent applications owned by third parties that cover certain other therapeutic uses of cytisine. We are currently monitoring these patents and patent applications. We may in the future pursue available proceedings in the U.S. and foreign patent offices to challenge the validity of these patents and patent applications. In addition, or alternatively, we may consider whether to seek to negotiate a license of rights to technology covered by one or more of such patents and patent applications for these certain additional therapeutic uses. If any third party patents or patent applications cover our product candidates or technologies in other therapeutic uses, we may not be free to manufacture or market our product candidates for additional therapeutic uses, absent such a license, which may not be available to us on commercially reasonable terms, or at all.
It is also possible that we have failed to identify relevant third-party patents or applications. For example, applications filed before November 29, 2000 and applications filed after that date that will not be filed outside the United States remain confidential until patents issue. Moreover, it is difficult for industry participants, including us, to identify all third-party patent rights that may be relevant to our product candidates and technologies because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. We may fail to identify relevant patents or patent applications or may identify pending patent applications of potential interest but incorrectly predict the likelihood that such
32
patent applications may issue with claims of relevance to our technology. In addition, we may be unaware of one or more issued patents that would be infringed by the manufacture, sale or use of a current or future product candidate, or we may incorrectly conclude that a third-party patent is invalid, unenforceable or not infringed by our activities. Additionally, pending patent applications that have been published can, subject to specified limitations, be later amended in a manner that could cover our technologies, our product candidates or the use of our product candidates.
There have been many lawsuits and other proceedings involving patent and other intellectual property rights in the pharmaceutical industries, including patent infringement lawsuits, interferences, oppositions, and reexamination proceedings before the USPTO and corresponding foreign patent offices. U.S. and foreign issued patents and pending patent applications, which are owned by third parties, exist in the fields in which we are developing product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that our product candidates may be subject to claims of infringement of the patent rights of third parties.
Parties making claims against us may obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our product candidates. Defense of these claims, regardless of their merit, would involve substantial litigation expense and would be a substantial diversion of employee resources from our business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys’ fees for willful infringement, pay royalties, redesign our infringing products or obtain one or more licenses from third parties, which may be impossible or require substantial time and monetary expenditure.
We intend to rely on patent rights for certain aspects of our product candidates and certain future product candidates. If we are unable to obtain or maintain an adequate proprietary position from this approach, we may not be able to compete effectively in our markets.
Although we rely or will rely primarily on trade secret protection as part of our intellectual property rights strategies, we also intend to rely on patent rights to protect certain aspects of our technologies and upon the patent rights of third parties from which we license certain of our technologies.
We have sought to protect our proprietary position by filing patent applications in the United Kingdom and intend to file patent applications in the United States related to future product candidates. This process is expensive and time consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner or at all. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection.
The patent position of pharmaceutical companies generally is highly uncertain and involves complex legal and factual questions for which legal principles remain unsolved. The patent applications that we own may fail to result in issued patents with claims that cover our product candidates in the United States or in other foreign countries. There is no assurance that all potentially relevant prior art relating to our patent applications or our patents (once issued) have been found, which can invalidate a patent or prevent a patent from issuing from a pending patent application. Even if patents do successfully issue, and even if such patents cover our future product candidates, third parties may challenge their validity, enforceability, or scope, which may result in such patents being narrowed, found unenforceable or invalidated. Furthermore, even if they are unchallenged, our patents and patent applications may not adequately protect our intellectual property, provide exclusivity for our future product candidates, or prevent others from designing around our claims. Any of these outcomes could impair our ability to prevent competition from third parties, which may have an adverse impact on our business.
We cannot offer any assurances about which, if any, patents will issue, the breadth of any such patent or whether any issued patents will be found invalid and unenforceable or will be threatened by third parties. Any successful opposition to these patents or any other patents owned by or licensed to us after patent issuance could deprive us of rights necessary for the successful commercialization of any future product candidates that we may develop. Further, if we encounter delays in regulatory approvals, the period of time during which we could market a future product candidate under patent protection could be reduced.
If we cannot obtain and maintain effective protection of exclusivity from our regulatory efforts and intellectual property rights, including patent protection or data exclusivity, for our product candidates, we may not be able to compete effectively and our business and results of operations would be harmed.
33
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect our product candidates.
Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal complexity, and is therefore costly, time-consuming, and inherently uncertain. In addition, the United States has recently enacted and is currently implementing wide-ranging patent reform legislation. Recent U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained, if any. Depending on decisions by the U.S. Congress, the federal courts and the U.S. Patent and Trademark Office, or the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future.
In a recent case, Assoc. for Molecular Pathology v. Myriad Genetics, Inc., the U.S. Supreme Court held that certain claims to naturally-occurring substances are not patentable. Cytisine is a naturally-occurring product and is not patentable. Our intellectual property strategy involves novel formulations of cytisine and there is no guarantee that such patents will be issued or if issued, will be broad enough to prevent competitors from developing competing cytisine products. Although we do not believe that any patents that may issue from our pending patent applications directed at our product candidates, if issued in their currently pending forms, as well as patent rights licensed by us, will be found invalid based on this decision, we cannot predict how future decisions by the courts, the U.S. Congress or the USPTO may impact the value of our patent rights. There could be similar changes in the laws of foreign jurisdictions that may impact the value of our patent rights or our other intellectual property rights.
We may be subject to claims that our employees, consultants, or independent contractors have wrongfully used or disclosed confidential information of third parties or that our employees have wrongfully used or disclosed alleged trade secrets of their former employers.
We employ individuals who were previously employed at other biotechnology or pharmaceutical companies. Although we have written agreements and make every effort to ensure that our employees, consultants, and independent contractors do not use the proprietary information or intellectual property rights of others in their work for us, we may in the future be subject to any claims that our employees, consultants, or independent contractors have wrongfully used or disclosed confidential information of third parties. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel, which could adversely impact our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Risks Related to our Common Stock
The price for our common stock is volatile.
The market prices for our common stock and that of early-stage pharmaceutical, biotechnology and other life sciences companies have historically been particularly volatile. Some of the factors that may cause the market price of our common stock to fluctuate include:
|
|
• |
the ability of us or our partners to develop cytisine and other product candidates and conduct clinical trials that demonstrate such product candidates are safe and effective; |
|
|
• |
our ability to raise additional capital, the terms of such capital, and our ability to continue as a going concern; |
|
|
• |
our ability or our partners to obtain regulatory approvals for cytisine or other product candidates, and delays or failures to obtain such approvals; |
|
|
• |
failure of any of our product candidates to demonstrate safety and efficacy, receive regulatory approval and achieve commercial success; |
|
|
• |
failure to maintain our existing third party license, manufacturing and supply agreements; |
|
|
• |
failure by us or our licensors to prosecute, maintain, or enforce our intellectual property rights; |
|
|
• |
changes in laws or regulations applicable to our candidates; |
|
|
• |
any inability to obtain adequate supply of product candidates or the inability to do so at acceptable prices; |
|
|
• |
adverse regulatory authority decisions; |
|
|
• |
introduction of new or competing products by our competitors; |
34
|
|
• |
the perception of the pharmaceutical industry by the public, legislatures, regulators and the investment community; |
|
|
• |
announcements of significant acquisitions, strategic partnerships, joint ventures, or capital commitments by us or our competitors; |
|
|
• |
disputes or other developments relating to proprietary rights, including patents, litigation matters, and our ability to obtain intellectual property protection for our technologies; |
|
|
• |
additions or departures of key personnel; |
|
|
• |
significant lawsuits, including intellectual property or stockholder litigation; |
|
|
• |
if securities or industry analysts do not publish research or reports about us, or if they issue an adverse or misleading opinions regarding our business and stock; |
|
|
• |
changes in the market valuations of similar companies; |
|
|
• |
general market or macroeconomic conditions; |
|
|
• |
sales of our common stock us or our stockholders in the future; |
|
|
• |
trading volume of our common stock; |
|
|
• |
adverse publicity relating to our markets generally, including with respect to other products and potential products in such markets; |
|
|
• |
changes in the structure of health care payment systems; and |
|
|
• |
period-to-period fluctuations in our financial results. |
Moreover, the stock markets in general have experienced substantial volatility that has often been unrelated to the operating performance of individual companies. These broad market fluctuations may also adversely affect the trading price of our common stock. An increase in the market price of our common stock, which is uncertain and unpredictable, may be the sole source of gain from an investment in our common stock. An investment in our common stock may not be appropriate for investors who require dividend income. We have never declared or paid cash dividends on our capital stock and do not anticipate paying any cash dividends on our capital stock in the foreseeable future. We currently intend to retain all available funds and any future earnings to fund the development and growth of our business. As a result, capital appreciation, if any, of our common stock will be the sole source of gain for stockholders for the foreseeable future. Accordingly, an investment in our common stock may not be appropriate for investors who require dividend income or investors who are not prepared to bear a significant risk of losses from such an investment.
We are at risk of securities class action litigation.
In the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities, including in circumstances where such declines occur in close proximity to the announcement of clinical trial results. Additionally, our stock price and those of other biotechnology and biopharmaceutical companies have experienced significant stock price volatility in recent years. If we face such litigation, it could result in substantial costs and a diversion of management’s attention and resources, which could harm our business.
If the ownership of our common stock is highly concentrated, it may prevent you and other stockholders from influencing significant corporate decisions and may result in conflicts of interest that could cause our stock price to decline.
Executive officers and directors and their affiliates beneficially own or control a significant percentage of the outstanding shares of our common stock. Accordingly, these executive officers, directors and their affiliates, acting as a group, will have substantial influence over the outcome of corporate actions requiring stockholder approval, including the election of directors, any merger, consolidation or sale of all or substantially all of our assets or any other significant corporate transactions. These stockholders may also delay or prevent a change of control, even if such a change of control would benefit the other stockholders. The significant concentration of stock ownership may adversely affect the trading price of our common stock due to investors’ perception that conflicts of interest may exist or arise
35
Because our recent merger resulted in an ownership change under Section 382 of the Code for OncoGenex, pre-merger net operating loss carryforwards and certain other tax attributes are now subject to limitations.
If a corporation undergoes an “ownership change” within the meaning of Section 382 of the Code, the corporation’s net operating loss carryforwards and certain other tax attributes arising from before the ownership change are subject to limitations on use after the ownership change. In general, an ownership change occurs if there is a cumulative change in the corporation’s equity ownership by certain stockholders that exceeds fifty percentage points over a rolling three-year period. Similar rules may apply under state tax laws. Our recent merger involving OncoGenex and Achieve Life Sciences, Inc. resulted in an ownership change for OncoGenex and, accordingly, OncoGenex’s net operating loss carryforwards and certain other tax attributes will be subject to limitations on their use after the merger. Additional ownership changes in the future could result in additional limitations on the combined organization’s net operating loss carryforwards. Consequently, even if we achieve profitability, we may not be able to utilize a material portion of our net operating loss carryforwards and other tax attributes, which could have a material adverse effect on cash flow and results of operations.
Anti-takeover provisions under Delaware law could make an acquisition of us more difficult and may prevent attempts by our stockholders to replace or remove our management.
Because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporate Law, which prohibits stockholders owning in excess of 15% of our outstanding voting stock from merging or combining with us. Although we believe these provisions collectively will provide for an opportunity to receive higher bids by requiring potential acquirors to negotiate with our board of directors, they would apply even if the offer may be considered beneficial by some stockholders. In addition, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove then current management by making it more difficult for stockholders to replace members of the board of directors, which is responsible for appointing the members of management.
Our bylaws provide that the Court of Chancery of the State of Delaware is the exclusive forum for substantially all disputes between us and our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us or our directors, officers or other employees.
Our bylaws provide that the Court of Chancery of the State of Delaware is the sole and exclusive forum for any derivative action or proceeding brought on our behalf, any action asserting a breach of fiduciary duty owed by any of our directors, officers or other employees to us or our stockholders, any action asserting a claim against us arising pursuant to any provisions of the Delaware General Corporation Law, our certificate of incorporation or our bylaws, or any action asserting a claim against us that is governed by the internal affairs doctrine. The choice of forum provision may limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes with us or our directors, officers or other employees, which may discourage such lawsuits against us and our directors, officers and other employees. If a court were to find the choice of forum provision contained in the bylaws to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving such action in other jurisdictions.
The sale of additional shares of common stock to LPC may cause the price of our common stock to decline and result in dilution to our existing stockholders.
Pursuant to our purchase agreement with LPC, we have the right, from time to time, in our sole discretion and subject to certain conditions, to direct LPC to purchase additional shares of common stock having an aggregate value of $10.0 million and we have exercised this right. We have directed LPC to purchase additional shares and may further direct LPC to purchase additional shares as often as every business day over the 30-month term of the Purchase Agreement in increments of up to 80,000 shares of common stock, with such amounts increasing as the closing sale price of our common stock increases. The purchase price of shares of common stock pursuant to the Purchase Agreement have been and will be based on prevailing market prices of common stock at the time of sale without any fixed discount, and we have controlled and will control the timing and amount of any sales of common stock to LPC. In addition, we have directed and we may direct LPC in the future to purchase additional amounts as accelerated purchases if on the date of a regular purchase the closing sale price of the common stock is not below $2.00 per share. The sale of additional shares of our common stock pursuant to our purchase agreement with LPC has or will have a dilutive impact on our existing stockholders. Sales by us to LPC could cause the market price of our common stock to decline significantly. Sales of our common stock under the purchase agreement, or the perception that such sales will occur, could also encourage short sales by third parties, which could contribute to the further decline of our stock price. Additionally, the sale of a substantial number of shares of our common stock under the purchase agreement, or the perception that such sales will occur, could make it more difficult for us to sell equity or equity-related securities in the future at a time and at a price that we might otherwise wish.
36
If we raise additional capital, the terms of the financing transactions may cause dilution to existing stockholders or contain terms that are not favorable to us.
In the future, we may seek to raise additional financing through private placements or public offerings of our equity or debt securities. We cannot be certain that additional funding will be available on acceptable terms, if at all. To the extent that we raise additional financing by issuing equity securities, we may do so at a price per share that represents a discount to the then-current per share trading price of our common stock and our stockholders may experience significant dilution. Any debt financing, if available, may involve restrictive covenants, such as limitations on our ability to incur additional indebtedness, limitations on our ability to acquire or license intellectual property rights and other operating restrictions that could adversely affect our ability to conduct our business.
None.
We have business offices located in Seattle, Washington and Vancouver, British Columbia.
Our lease agreement for office space in Bothell, Washington commenced on February 15, 2015 and had a three-year term with one three-year renewal option. Pursuant to this lease, we rented approximately 13,771 square feet of office space. The annual rent was approximately $0.3 million. We did not exercise our renewal option under the lease agreement and the lease expires on April 30, 2018.
On December 11, 2017, we entered into a lease agreement for office space in Seattle, Washington, which commenced on March 1, 2018, and will expire at the end of the month on the third anniversary of the lease. Pursuant to this lease, we rent approximately 3,187 square feet of office space. The annual rent is approximately $0.1 million.
We lease approximately 4,857 square feet in Vancouver, British Columbia, currently at an annual rent of approximately CND $0.1 million, which lease expires on September 30, 2018.
We believe that the facilities we currently lease are sufficient for our anticipated near-term needs.
From time to time, we may be involved in litigation relating to claims arising out of our operations in the normal course of business. We are not currently a party to any legal proceedings, the adverse outcome of which, in management’s opinion, individually or in the aggregate, would have a material adverse effect on the results of our operations or financial position. There are no material proceedings to which any director, officer or any of our affiliates, any owner of record or beneficially of more than five percent of any class of our voting securities, or any associate of any such director, officer, our affiliates, or security holder, is a party adverse to us or our consolidated subsidiary or has a material interest adverse thereto.
Not applicable.
37
|
MARKET FOR THE REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Our common stock first began trading on the Nasdaq National Market under the symbol “SNUS” on October 12, 1995. In connection with a corporate transaction and name change, our common stock commenced trading on the Nasdaq Capital Market under the stock symbol “OGXI”, effective August 21, 2008. Following the completion of the Arrangement discussed elsewhere in this Annual Report on Form 10-K, our common stock commenced trading on the Nasdaq Capital Market under the stock symbol “ACHV”, effective August 2, 2017.
No cash dividends have been paid on our common stock, and we do not anticipate paying any cash dividends in the foreseeable future. As of February 15, 2018, there were approximately 53 stockholders of record and there were approximately 8,232 beneficial stockholders of our common stock. The high and low sales prices of our common stock as reported by the NASDAQ Capital Market for the periods indicated are as follows:
|
Achieve Life Sciences, Inc. |
|
HIGH |
|
|
LOW |
|
||
|
|
|
|
|
|
|
|
|
|
|
YEAR ENDED DECEMBER 31, 2016: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First quarter |
|
$ |
13.53 |
|
|
$ |
5.01 |
|
|
Second quarter |
|
|
15.62 |
|
|
|
7.48 |
|
|
Third quarter |
|
|
11.33 |
|
|
|
5.06 |
|
|
Fourth quarter |
|
|
7.72 |
|
|
|
3.64 |
|
|
|
|
|
|
|
|
|
|
|
|
YEAR ENDED DECEMBER 31, 2017: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First quarter |
|
$ |
10.18 |
|
|
$ |
4.73 |
|
|
Second quarter |
|
|
5.06 |
|
|
|
3.61 |
|
|
Third quarter |
|
|
6.27 |
|
|
|
2.03 |
|
|
Fourth quarter |
|
|
3.85 |
|
|
|
1.15 |
|
|
(1) |
|
All amounts reported herein are presented on a post-one-for-eleven reverse stock split basis. |
The information required by this item regarding equity compensation plan information is set forth in Part III, Item 12 of this Annual Report on Form 10-K. No purchases of equity securities during the year ended December 31, 2017 were made by us or on our behalf and we did not sell any unregistered securities during such year.
38
The following performance graph shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or incorporated by reference into any of our filings under the Securities Act or the Exchange Act, except as expressly set forth by specific reference in such filings. The graph compares the cumulative five-year total return provided to stockholders on our common stock relative to the cumulative total returns of the NASDAQ Composite Index and the NASDAQ Pharmaceutical Index. An investment of $100 (with reinvestment of all dividends into additional shares of the same class of equity securities at the frequency with which dividends are paid on such securities during the applicable year) is assumed to have been made in our common stock and in each of the indexes on December 31, 2012 and its relative performance is tracked through December 31, 2017.
The stock price performance included in this graph is not necessarily indicative of future stock price performance.
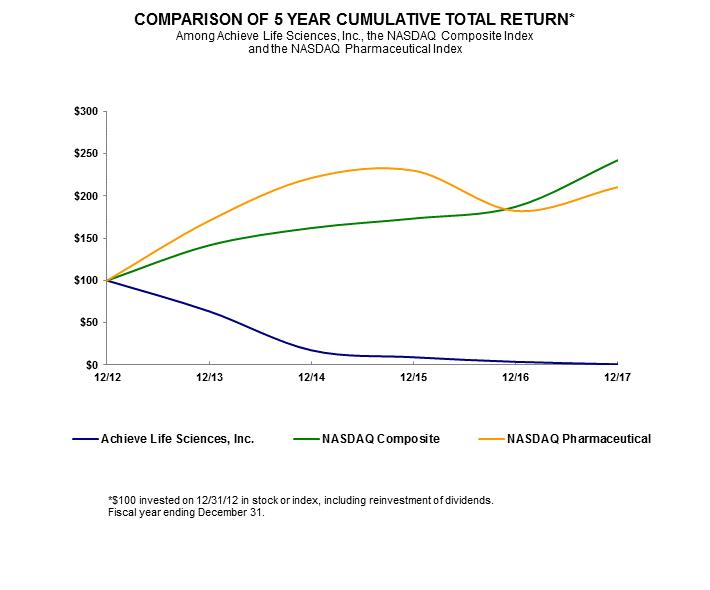
|
|
|
12/31/12 |
|
|
12/31/13 |
|
|
12/31/14 |
|
|
12/31/15 |
|
|
12/31/16 |
|
|
12/31/17 |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Achieve Life Sciences, Inc. |
|
|
100.00 |
|
|
|
63.57 |
|
|
|
17.45 |
|
|
|
9.22 |
|
|
|
3.81 |
|
|
|
0.93 |
|
|
NASDAQ Composite |
|
|
100.00 |
|
|
|
141.63 |
|
|
|
162.09 |
|
|
|
173.33 |
|
|
|
187.19 |
|
|
|
242.29 |
|
|
NASDAQ Pharmaceutical |
|
|
100.00 |
|
|
|
170.57 |
|
|
|
221.26 |
|
|
|
229.97 |
|
|
|
182.33 |
|
|
|
210.44 |
|
39
The data set forth below should be read in conjunction with Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and the Consolidated Financial Statements and Notes thereto appearing at Item 8 of this Annual Report on Form 10-K. The selected consolidated statements of loss data for the years ended December 31, 2017, 2016 and 2015 and consolidated balance sheet data as of December 31, 2017 and 2016 set forth below have been derived from our audited consolidated financial statements included elsewhere in this Annual Report on Form 10-K. The selected statements balance sheet data as of December 31, 2015 set forth below have been derived from the audited consolidated financial statements for such years not included in this Annual Report on Form 10-K.
In connection with the Arrangement, Achieve was considered to be the acquiring company for accounting purposes. Accordingly, the assets and liabilities of OncoGenex were recorded, as of the effective time of the Arrangement, at their respective fair values and added to those of Achieve. The results of the operations and balance sheet data for the year ended December 31, 2017 reflect the results of only Achieve for the time period of January 1, 2017 through August 1, 2017 and the results of the combined company from August 2, 2017 through December 31, 2017. The historical results of operations and balance sheet data shown for years ended December 31, 2016 and 2015 reflect only those of Achieve prior to the Arrangement, and do not reflect the results of OncoGenex. The historical results presented are not necessarily indicative of future results.
|
|
|
December 31, |
|
|||||||||
|
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
|||
|
|
|
(in thousands except share and per share amounts) |
|
|||||||||
|
Statements of Loss Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total expenses |
|
$ |
6,632 |
|
|
$ |
1,714 |
|
|
$ |
1,223 |
|
|
Net loss |
|
$ |
(10,583 |
) |
|
$ |
(1,234 |
) |
|
$ |
(828 |
) |
|
Basic and diluted loss per common share |
|
$ |
(2.21 |
) |
|
$ |
(58.13 |
) |
|
$ |
(39.00 |
) |
|
Shares used in calculation of net loss per share |
|
|
|
|
|
|
|
|
|
|
|
|
|
Basic and diluted |
|
|
4,794,421 |
|
|
|
21,230 |
|
|
|
21,230 |
|
|
|
|
December 31, |
|
|||||||||
|
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
|||
|
|
|
(in thousands) |
|
|||||||||
|
Balance Sheet Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash, cash equivalents and short-term investments |
|
$ |
5,284 |
|
|
$ |
15 |
|
|
$ |
67 |
|
|
Total assets |
|
$ |
9,892 |
|
|
$ |
3,807 |
|
|
$ |
4,078 |
|
|
Current liabilities |
|
$ |
2,013 |
|
|
$ |
3,073 |
|
|
$ |
1,611 |
|
|
Total liabilities |
|
$ |
2,013 |
|
|
$ |
3,197 |
|
|
$ |
2,238 |
|
|
Additional paid-in capital |
|
$ |
20,556 |
|
|
$ |
2,667 |
|
|
$ |
2,667 |
|
|
Accumulated deficit |
|
$ |
(12,694 |
) |
|
$ |
(2,062 |
) |
|
$ |
(828 |
) |
|
Stockholders’ equity |
|
$ |
7,879 |
|
|
$ |
610 |
|
|
$ |
1,840 |
|
40
Forward-Looking Statements
This Annual Report on Form 10-K contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. These forward-looking statements involve a number of risks and uncertainties. We caution readers that any forward-looking statement is not a guarantee of future performance and that actual results could differ materially from those contained in the forward-looking statement. These statements are based on current expectations of future events. Such statements include, but are not limited to, statements about future financial and operating results, plans, objectives, expectations and intentions, costs and expenses, interest rates, outcome of contingencies, financial condition, results of operations, liquidity, business strategies, cost savings, objectives of management and other statements that are not historical facts. You can find many of these statements by looking for words like “believes,” “expects,” “anticipates,” “estimates,” “may,” “should,” “will,” “could,” “plan,” “intend,” or similar expressions in this Annual Report on Form 10-K or in documents incorporated by reference into this Annual Report on Form 10-K . We intend that such forward-looking statements be subject to the safe harbors created thereby. Examples of these forward-looking statements include, but are not limited to:
|
|
• |
our ability to continue as a going concern, our anticipated future capital requirements and the terms of any capital financing agreements; |
|
|
• |
progress and preliminary and future results of any clinical trials; |
|
|
• |
anticipated regulatory filings, requirements and future clinical trials; |
|
|
• |
timing and amount of future contractual payments, product revenue and operating expenses; and |
|
|
• |
market acceptance of our products and the estimated potential size of these markets. |
These forward-looking statements are based on the current beliefs and expectations of our management and are subject to significant risks and uncertainties. If underlying assumptions prove inaccurate or unknown risks or uncertainties materialize, actual results may differ materially from current expectations and projections. Factors that might cause such a difference include those discussed in Item 1A “Risk Factors,” as well as those discussed elsewhere in the Annual Report on Form 10-K.
You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this Annual Report on Form 10-K or, in the case of documents referred to or incorporated by reference, the date of those documents.
All subsequent written or oral forward-looking statements attributable to us or any person acting on our behalf are expressly qualified in their entirety by the cautionary statements contained or referred to in this section. We do not undertake any obligation to release publicly any revisions to these forward-looking statements to reflect events or circumstances after the date of this Annual Report on Form 10-K or to reflect the occurrence of unanticipated events, except as may be required under applicable U.S. securities law. If we do update one or more forward-looking statements, no inference should be drawn that we will make additional updates with respect to those or other forward-looking statements.
Overview
We are a clinical-stage pharmaceutical company committed to the global development and commercialization of cytisine for smoking cessation. Our focus is to address the global smoking health epidemic, which is a leading cause of preventable death and is responsible for approximately six million deaths annually worldwide.
Cytisine is an established 25-day smoking cessation treatment that has been approved and marketed in Central and Eastern Europe by Sopharma AD for over 20 years under the brand name TabexTM. It is estimated that over 20 million people have used cytisine to help treat nicotine addiction, including over 2,000 patients in investigator-conducted, Phase 3 clinical trials in Europe and New Zealand. Both trials were published in the New England Journal of Medicine in September 2011 and December 2014, respectively.
Cytisine is a naturally occurring, plant-based alkaloid from the seeds of the Laburnum anagyroides plant. Cytisine is structurally similar to nicotine and has a well-defined, dual-acting mechanism of action that is both agonistic and antagonistic. It is believed to aid in smoking cessation by interacting with nicotine receptors in the brain by reducing the severity of nicotine withdrawal symptoms through agonistic binding to nicotine receptors and by reducing the reward and satisfaction associated with smoking through antagonistic properties. The cytisine dosing schedule reflects that of an anti-addiction medication, with downward dose titration over a period of 25 days.
41
In late June 2017, we filed our Investigational New Drug, or IND, application for cytisine with the FDA, which included NCCIH sponsored non-clinical studies. The IND was accepted in late July 2017.
In August 2017, we initiated a study evaluating the effect of food on the bioavailability of cytisine in normal healthy volunteers. We completed the food effect study and announced the results in November of 2017 demonstrating similar bioavailability of cytisine in fed and fasted subjects.
In October 2017, we initiated a study assessing the repeat-dose Pharmacokinetics, or PK, and Pharmacodynamics, or PD, effects of 1.5mg and 3mg cytisine in 36 healthy volunteer smokers aged 18-65 years when administered over the standard 25-day course of treatment. Preliminary results on 24 smokers were announced in February 2018. The PK results indicated expected increases in plasma concentration with higher doses of cytisine. Smokers in the study were not required to have a designated or predetermined quit date, however, 58% of the subjects in the trial achieved biochemically verified smoking abstinence by day 26. Half (6/12) of the subjects on the 1.5mg arm and 67% (8/12) of the subjects on the 3.0mg arm achieved abstinence on day 26. Subjects who did not achieve abstinence had a significant reduction in number of daily cigarettes smoked by day 26. The adverse events observed were mostly mild with transient headaches as the most commonly reported event. No serious adverse events were observed in the study.
In December 2017, we submitted a meeting request to hold a pre-Phase 3 meeting with the FDA to review our Phase 3 program and overall development plans for cytisine. We received confirmation from the FDA for a meeting date in the second quarter of 2018. We intend to commence a Phase 3 clinical program in mid-2018, subject to FDA guidance and the availability of capital. In addition to the Phase 3 program, we expect to run additional supportive clinical studies including, but not limited to urine excretion, renal impairment and QT interval prolongation studies as well as supportive New Drug Application, or NDA, non-clinical chronic toxicity and carcinogenicity studies.
While third party trials of cytisine have been conducted that may inform future Company-sponsored clinical trials, we have not yet conducted any large scale company-sponsored clinical trials for cytisine in the United States or any other jurisdiction.
We previously were developing apatorsen, of which we discontinued further development in August 2017. We provided a notice of discontinuance to our former development partners for apatorsen, Ionis Pharmaceuticals, Inc., or Ionis, and a letter of termination to the University of British Columbia, or UBC, notifying them that we have discontinued development of apatorsen resulting in termination of all licensing agreements related to this product candidate. We believe that all financial obligations, other than continuing mutual indemnification obligations and our requirement to pay for out-of-pocket patent expenses incurred up to the date of termination and for abandoning the apatorsen patents and patent applications, under all apatorsen related agreements with Ionis and UBC, are no longer owed and no further payments are due.
Our management team has significant experience in growing emerging companies focused on the development of under-utilized pharmaceutical compounds to meet unmet medical needs. We intend to use this experience to develop and ultimately commercialize cytisine either directly or via strategic collaborations.
We have no products approved for commercial sale and have not generated any revenue from product sales to date. We have never been profitable and have incurred operating losses in each year since inception. Our net loss was $10.6 million for the year ended December 31, 2017, and $1.2 million for the year ended December 31, 2016. As of December 31, 2017, we had an accumulated deficit of $12.7 million, cash and cash equivalents balance of $5.3 million and a positive working capital balance of $3.7 million. Substantially all of our operating losses resulted from expenses incurred from general and administrative costs associated with our operations and research and development costs from our clinical development programs.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our ability to obtain additional financing. We expect to incur significant expenses and increasing operating losses for at least the next several years as we continue our clinical development of, and seek regulatory approval for, cytisine and add personnel necessary to operate as a public company with an advanced clinical candidate. We expect that our operating losses will fluctuate significantly from quarter to quarter and year to year due to timing of clinical development programs and efforts to achieve regulatory approval. Without additional funds, we may be forced to delay, scale back or eliminate some of our research and development activities or other operations and potentially delay product development in an effort to provide sufficient funds to continue our operations. If any of these events occurs, our ability to achieve our development and commercialization goals would be adversely affected.
Our current capital resources are insufficient to fund our planned operations for the next 12 months. We will continue to require substantial additional capital to continue our clinical development activities. Accordingly, we will need to raise substantial additional capital to continue to fund our operations from the sale of our securities, partnering arrangements or other financing transactions in order to finance the commercialization of our product candidates. The amount and timing of our future funding requirements will
42
depend on many factors, including the pace and results of our clinical development efforts. Failure to raise capital as and when needed, on favorable terms or at all, will have a negative impact on our financial condition and our ability to develop our product candidate.
The accompanying financial results have been prepared assuming we will continue to operate as a going concern, which contemplates the realization of assets and liabilities and commitments in the normal course of business. The financial results do not include any adjustments to the amounts and classification of assets and liabilities that might be necessary should we be unable to continue as a going concern. Such adjustments could be material.
Recent Corporate History
On August 1, 2017, OncoGenex Pharmaceuticals, Inc., or OncoGenex, completed a transaction, or the Arrangement, with Achieve Life Science, Inc., or Achieve, as contemplated by the Merger Agreement between Achieve and OncoGenex dated January 5, 2017, or the Merger Agreement. Under the terms of the Merger Agreement, OncoGenex changed its name to Achieve Life Sciences, Inc., instituted an one-for-eleven reverse stock split, issued 8,210,118 shares of its common stock (after accounting for the elimination of resulting fractional shares) in exchange for all of the outstanding preferred shares, common shares and convertible debentures of Achieve, and as a result Achieve became a wholly-owned subsidiary of OncoGenex, and is listed on the Nasdaq Capital Market under the ticker symbol ACHV. More information concerning the Arrangement is contained in our Current Report on Form 8-K filed on August 2, 2017 and our Amendment No. 3 to the Registration Statement on Form S-4/A filed with the SEC on June 6, 2017.
These consolidated financial statements account for the Arrangement between OncoGenex and Achieve as a reverse merger, whereby Achieve is deemed to be the acquiring entity from an accounting perspective. Our consolidated results of operations for the year ended December 31, 2017 include the results of operations of only Achieve for the time period of January 1, 2017 through August 1, 2017 and include the results of the combined company following the completion of the Arrangement on August 1, 2017. The consolidated results of operations for the years ended December 31, 2016 and December 31, 2015 include only the consolidated results of operations of Achieve and do not include historical results of OncoGenex. This treatment and presentation is in accordance with ASC 805, “Business Combinations”. Information relating to the number of shares, price per share and per share amounts of common stock are presented on a post- reverse stock split basis, as a reverse stock split in the ratio of one-for-eleven was effected in connection with the Arrangement.
In connection with the Arrangement, OncoGenex issued contingent value rights, or CVRs, on July 31, 2017 to their existing stockholders as of July 27, 2017. One CVR was issued for each share of their common stock outstanding as of the record date for such issuance. The CVRs expired on August 17, 2017. A recovery of $0.2 million was recognized on our Consolidated Statements of Loss and Comprehensive Loss.
License & Supply Agreements
Sopharma License and Supply Agreements
We are party to a license agreement, or the Sopharma License Agreement, and a supply agreement, or the Sopharma Supply Agreement, with Sopharma, AD, or Sopharma. Pursuant to the Sopharma License Agreement, we were granted access to all available manufacturing, efficacy and safety data related to cytisine, as well as a granted patent in several European countries related to new oral dosage forms of cytisine providing enhanced stability. Additional rights granted under the Sopharma License Agreement include the exclusive use of, and the right to sublicense, the trademark Tabex in all territories described in the Sopharma License Agreement. Under the Sopharma License Agreement, we agreed to pay a nonrefundable license fee. In addition, we agreed to make certain royalty payments equal to a mid-single digit percentage of all net sales of Tabex branded products in our territory during the term of the Sopharma License Agreement, including those sold by a third party pursuant to any sublicense which may be granted by us. To date, we have paid Sopharma $10 pursuant to the Sopharma License Agreement.
University of Bristol License Agreement
In July 2016, we entered into a license agreement with the University of Bristol, or the University of Bristol License Agreement. Under the University of Bristol License Agreement, we received exclusive and nonexclusive licenses from the University of Bristol to certain patent and technology rights resulting from research activities into cytisine and its derivatives, including a number of patent applications related to novel approaches to cytisine binding at the nicotinic receptor level.
In consideration of rights granted by the University of Bristol, we paid a nominal license fee and agreed to pay amounts of up to $3.2 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the University of Bristol License Agreement. Additionally, if we successfully commercialize product candidates subject to the University of Bristol License Agreement, we are responsible for royalty payments in the low-single
43
digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products.
On January 22, 2018, we and the University of Bristol entered into an amendment to the University of Bristol License Agreement. Pursuant to the amended University of Bristol License Agreement we received exclusive rights for all human medicinal uses of cytisine across all therapeutic categories from the University of Bristol from research activities into cytisine and its derivatives. In consideration of rights granted by the amended University of Bristol License Agreement, we agreed to pay an initial amount of $37,500 upon the execution of the amended University of Bristol License Agreement, and additional amounts of up to $1.7 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the amended University of Bristol License Agreement, in addition to amounts under the original University of Bristol License Agreement of up to $3.2 million in the aggregate, tied to specific financing, development and commercialization milestones. Additionally, if we successfully commercialize any product candidate subject to the amended University of Bristol License Agreement or to the original University of Bristol License Agreement, we will be responsible, as provided in the original University of Bristol License Agreement, for royalty payments in the low-single digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products. To date, we have paid the University of Bristol $50,000 pursuant to the University of Bristol License Agreement.
Research and Development Expenses
Research and development, or R&D, expenses consist primarily of costs for clinical trials, contract manufacturing, personnel costs, milestone payments to third parties, facilities, regulatory activities, preclinical studies and allocations of other R&D-related costs. External expenses for clinical trials include fees paid to clinical research organizations, clinical trial site costs and patient treatment costs.
We manage our clinical trials through contract research organizations and independent medical investigators at our sites and at hospitals and expect this practice to continue. Due to the number of projects and our ability to utilize resources across several projects, we do not record or maintain information regarding the indirect operating costs incurred for our research and development programs on a program-specific basis. In addition, we believe that allocating costs on the basis of time incurred by our employees does not accurately reflect the actual costs of a project.
We expect our research and development expenses to increase for the foreseeable future as we continue to conduct our ongoing pre-clinical studies, and initiate new clinical trials and registration-enabling activities. The process of conducting clinical trials and pre-clinical studies necessary to obtain regulatory approval is costly and time consuming and we may never succeed in achieving marketing approval for cytisine. (See “Item 1A. Risk Factors—Risks Related to the Development of Our Product Candidates.”)
Successful development of cytisine is highly uncertain and may not result in an approved product. We cannot estimate completion dates for development activities or when we might receive material net cash inflows from our R&D projects, if ever. We anticipate we will make determinations as to which markets, and therefore, which regulatory approvals, to pursue and how much funding to direct toward achieving regulatory approval in each market on an ongoing basis in response to our ability to enter into new strategic alliances with respect to each program or potential product candidate, the scientific and clinical success of each future product candidate, and ongoing assessments as to each future product candidate’s commercial potential. We will need to raise additional capital and may seek additional strategic alliances in the future in order to advance our various programs.
Our projects or intended R&D activities may be subject to change from time to time as we evaluate results from completed studies, our R&D priorities and available resources.
General and Administrative Expenses
General and administrative, or G&A, expenses consist primarily of salaries and related costs for our personnel in executive, finance and accounting, corporate communications and other administrative functions, as well as consulting costs, including market research, business consulting, human resources and intellectual property. Other costs include professional fees for legal and auditing services, insurance and facility costs.
44
The following is a summary of outstanding warrants to purchase common stock that are classified as liabilities at December 31, 2017:
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
Outstanding |
|
|
Exercise |
|
|
|
||
|
|
|
and |
|
|
price per |
|
|
|
||
|
|
|
Exercisable |
|
|
Share |
|
|
Expiration Date |
||
|
(1) Series A Warrants issued in July 2014 financing |
|
|
252,721 |
|
|
|
44.00 |
|
|
July 2019 |
|
(2) Series B Warrants issued in July 2014 financing |
|
|
60,933 |
|
|
|
44.00 |
|
|
July 2019 |
No warrants classified as liabilities were exercised during the years ended December 31, 2017 or 2016.
We reassess the fair value of the common stock warrants classified as liabilities at each reporting date utilizing a Black-Scholes pricing model. Inputs used in the pricing model include estimates of stock price volatility, expected warrant life and risk-free interest rate. The computation of expected volatility was based on the historical volatility of comparable companies from a representative peer group selected based on industry and market capitalization.
Results of Operations
Years Ended December 31, 2017, 2016 and 2015
Research and Development Expenses
Our research and development expenses for our clinical development programs were as follows (in thousands):
|
|
|
Year ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
|||
|
Clinical development programs: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cytisine |
|
$ |
1,590 |
|
|
$ |
286 |
|
|
$ |
107 |
|
|
Other research and development |
|
|
1,511 |
|
|
|
— |
|
|
|
— |
|
|
Total research and development expenses |
|
$ |
3,101 |
|
|
$ |
286 |
|
|
$ |
107 |
|
Research and development expenses for the years ended December 31, 2017, 2016 and 2015 were $3.1 million, $0.3 million and $0.1 million, respectively. The increase in 2017 as compared to 2016 was due to increased research and development activity for our cytisine clinical development program, including the costs associated with filing the IND application, initiating and completing the food effects trial, initiating the repeat dose pharmacokinetics trial and initiating toxicology studies and increased employee expenses and higher facilities costs resulting from the reverse merger of OncoGenex. The increase in research and development expenses in 2016 as compared to 2015 was primarily related to increased activity in connection with coordinating regulatory and clinical development activities with the FDA, European Medicines Agency, or EMA, and the National Institute of Health, or NIH, and non-clinical updates.
General and Administrative Expenses
G&A expenses for the years ended December 31, 2017, 2016 and 2015 were $3.5 million, $1.4 million and $1.1 million, respectively. The increase in 2017 as compared to 2016 was due to increase in employee headcount, consulting fees, legal fees and professional fees as a result of the closing of the Arrangement and the integration of OncoGenex with our operations. The increase in general and administrative expenses in 2016 as compared to 2015 was primarily related to the fact that the company was incorporated in May 2015 and did not operate for a full year during the period ended December 31, 2015
Gain / (loss) on warrants
We recorded a gain on the revaluation of our outstanding warrants for the year ended December 31, 2017 of $0.1 million, which is included on our consolidated statement of loss as a gain on warrants. We revalue the warrants at each balance sheet date to fair value. For the years ended December 31, 2016 and 2015 we did not have any outstanding warrants.
45
In accordance with ASC 805, “Business Combinations,” the excess of fair value of acquired net assets over purchase price (negative goodwill) of $1.3 million, was recognized as a gain in the period the Arrangement was completed. We have reassessed whether all acquired assets and assumed liabilities have been identified and recognized and performed remeasurements to verify that the consideration paid, assets acquired, and liabilities assumed have been properly valued.
Contingent value rights recovery
The contingent value rights issued by Oncogenex to its shareholders prior to the closing of the Arrangement, expired on August 17, 2017, as we did not enter into any term sheets or agreement with third parties for the development or commercialization of apatorsen. A recovery of $0.2 million was recognized on our Consolidated Statements of Loss and Comprehensive Loss.
Loss on disposition of intangible asset and Recovery of deferred income taxes
In August 2017, we discontinued further development of apatorsen. We recognized a loss on disposition of apatorsen of $8.6 million and a deferred income tax recovery of $2.9 million as a result of discontinuing the development program and providing a notice of discontinuance of the license agreements with Ionis.
Liquidity and Capital Resources
We have incurred an accumulated deficit of $12.7 million through December 31, 2017, and we expect to incur substantial additional losses in the future as we operate our business and continue or expand our R&D activities and other operations. We have not generated any revenue from product sales to date, and we may not generate product sales revenue in the near future, if ever. As of December 31, 2017, we had a cash and cash equivalents balance of $5.3 million and a positive working capital balance of $3.7 million.
The financial results have been prepared assuming we will continue to operate as a going concern, which contemplates the realization of assets and liabilities and commitments in the normal course of business.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our ability to obtain additional financing. There is no assurance that we will obtain financing from other sources. We have, thus far, financed our operations through the closing of the Arrangement and equity financing. Without additional funds, we may be forced to delay, scale back or eliminate some of our research and development activities or other operations and potentially delay product development in an effort to provide sufficient funds to continue our operations. If any of these events occurs, our ability to achieve our development and commercialization goals would be adversely affected.
Our current capital resources are insufficient to fund our planned operations for the next 12 months. We will continue to require substantial additional capital to continue our clinical development activities. Accordingly, we will need to raise substantial additional capital to continue to fund our operations from the sale of our securities, partnering arrangements or other financing transactions in order to finance the commercialization of our product candidates. The amount and timing of our future funding requirements will depend on many factors, including the pace and results of our clinical development efforts. Failure to raise capital as and when needed, on favorable terms or at all, will have a negative impact on our financial condition and our ability to develop our product candidate.
The consolidated financial results do not include any adjustments to the amounts and classification of assets and liabilities that might be necessary should we be unable to continue as a going concern. Such adjustments could be material.
On September 14, 2017, we and Lincoln Park Capital Fund, LLC, or LPC, entered into a share and unit purchase agreement, or Purchase Agreement, pursuant to which we have the right to sell to LPC up to $11.0 million in shares of our common stock, par value $0.001 per share, subject to certain limitations and conditions set forth in the Purchase Agreement.
Pursuant to the Purchase Agreement, LPC initially purchased 328,947 of our units, or the Units, purchase price of $3.04 per unit, with each Unit consisting of (a) one share of our Common Stock and (b) one warrant to purchase one-quarter of a share of Common Stock at an exercise price of $3.496 per share, or Warrant. Each Warrant is exercisable six months following the issuance date until the date that is five years and six months after the issuance date and is subject to customary adjustments. The Warrants were issued only as part of the Units in the initial purchase of $1.0 million and no warrants shall be issued in connection with any other purchases of common stock under the Purchase Agreement.
46
After the initial purchase, if our stock price is above $1.00, as often as every other business day over the 30-month term of the Purchase Agreement, and up to an aggregate amount of an additional $10.0 million (subject to certain limitations) of shares of common stock, we have the right, from time to time, in our sole discretion and subject to certain conditions to direct LPC to purchase up to 80,000 shares of common stock with such amounts increasing as the closing sale price of our common stock as reported on The NASDAQ Capital Market increases. The purchase price of shares of common stock pursuant to the Purchase Agreement will be based on prevailing market prices of common stock at the time of sales without any fixed discount, and we will control the timing and amount of any sales of common stock to LPC. In addition, we may direct LPC to purchase additional amounts as accelerated purchases if on the date of a regular purchase the closing sale price of the common stock is not below $2.00 per share. As consideration for entering into the Purchase Agreement, we issued to LPC 123,516 shares of common stock; no cash proceeds were received from the issuance of these shares.
From September 14, 2017 through March 1, 2018, we offered and sold 1,673,778 shares of our common stock pursuant to our Purchase Agreement with LPC, including the 328,947 shares that were part of the initial purchase of Units. These sales resulted in gross proceeds to us of approximately $3.4 million. As of March 1, 2018 shares of our common stock having an aggregate value of approximately $7.6 million remained available for sale under this offering program.
Cash Flows
Operating Activities
For the years ended December 31, 2017, 2016 and 2015, net cash used in operating activities was $9.1 million, $0.2 million, and $0.4 million, respectively. The increase in cash used in operations in 2017 as compared to 2016 was primarily attributable to increased personnel and facilities assumed in the Arrangement, increased research and development expenses for our cytisine development program and cash used to reduce liabilities assumed in the Arrangement. The decrease in cash used in operating activities in 2016 as compared to 2015 was primarily attributable to increases in accrued liabilities and accrued compensation during the year ended December 31, 2016.
Financing Activities
For the years ended December 31, 2017, 2016 and 2015 net cash provided by financing activities was $2.0 million, $0.2 million and $2.4 million, respectively Net cash provided by financing activities for the year ended December 31, 2017 relates to proceeds received from our purchase agreement with LPC. Net cash provided by financing activities for the year ended December 31, 2016 related to proceeds from promissory notes payable to a certain shareholder. Net cash provided by financing activities for the year ended December 31, 2015 related to proceeds from a $2.0 million convertible promissory note and a $0.7 million promissory note payable to a certain shareholder, offset by a $0.3 million loan payment to Sopharma, AD.
Investing Activities
Net cash provided by financing activities for the years ended December 31, 2017 and 2016 was $12.6 million and zero, respectively. Net cash used in investing activities for the year ended December 31, 2015 was $2.0 million. Net cash provided by investing activities for the year ended December 31, 2017 was due to the reverse merger with OncoGenex. There were no investing activities for the year ended December 31, 2016. Net cash used in investing activities for the year ended December 31, 2015 related to the purchase price for the acquisition of Extab Corporation.
Contractual Obligations
The following table summarizes our contractual obligations as of December 31, 2017 (in thousands):
|
|
|
Total |
|
|
Less than 1 year |
|
|
1-3 years |
|
|
3-5 years |
|
|
More than 5 years |
|
|||||
|
Bothell office operating lease (1) |
|
$ |
95 |
|
|
$ |
95 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Vancouver office operating lease (2) |
|
$ |
71 |
|
|
$ |
71 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Seattle office operating lease (3) |
|
$ |
433 |
|
|
$ |
117 |
|
|
$ |
291 |
|
|
$ |
25 |
|
|
$ |
— |
|
|
Leased equipment |
|
$ |
3 |
|
|
$ |
3 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Total |
|
$ |
602 |
|
|
$ |
286 |
|
|
$ |
291 |
|
|
$ |
25 |
|
|
$ |
— |
|
47
|
(1) |
This operating lease is effective May 1, 2015 and expires on April 30, 2018. |
|
(2) |
This operating lease expires in 2018. |
|
(3) |
This operating lease is effective March 1, 2018 and expires on February 28, 2021. |
Off-Balance Sheet Arrangements
We do not have any off-balance sheet financing arrangements at December 31, 2017.
Inflation
We do not believe that inflation has had a material effect on our business and results of operations during the periods presented.
Material Changes in Financial Condition
|
|
|
December 31, |
|
|||||
|
(in thousands) |
|
2017 |
|
|
2016 |
|
||
|
Total Assets |
|
$ |
9,892 |
|
|
$ |
3,807 |
|
|
Total Liabilities |
|
|
2,013 |
|
|
|
3,197 |
|
|
Total Equity |
|
|
7,879 |
|
|
|
610 |
|
The increase in assets as at December 31, 2017 as compared to December 31, 2016 primarily relates to increase in cash and cash equivalents following the Arrangement. The decrease in liabilities as at December 31, 2017 compared to December 31, 2016 was primarily due to lower stockholder loans with related parties and lower accrued compensation.
Critical Accounting Policies and Estimates
Use of Estimates
The preparation of consolidated financial statements in conformity with United States generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and notes thereto. Actual results could differ from these estimates. Estimates and assumptions principally relate to estimates of the fair value of our warrant liability, the initial fair value and forfeiture rates of stock options issued to employees and consultants, the estimated compensation cost on performance restricted stock unit awards and clinical trial and manufacturing accruals, estimated useful lives of property, plant and equipment and estimates and assumptions in contingent liabilities.
Fair value of financial instruments
The fair value of our cash equivalents and marketable securities is based on quoted market prices and trade data for comparable securities. We determine the fair value of our warrant liability based on the Black-Scholes pricing model and using considerable judgment, including estimating stock price volatility and expected warrant life. Other financial instruments including amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities and accrued compensation are carried at cost, which we believe approximates fair value because of the short-term maturities of these instruments.
Intangible Assets
Our intangible assets are subject to amortization and are amortized using the straight-line method over their estimated period of benefit. We evaluate the carrying amount of intangible assets periodically by taking into account events or circumstances that may warrant revised estimates of useful lives or that indicate the asset may be impaired.
Impairment of Long-Lived Assets
We review long-lived assets for impairment whenever events or changes in circumstances indicate that the asset’s carrying amount may not be recoverable. We conduct our long-lived asset impairment analyses in accordance with ASC 360-10-15, “Impairment or Disposal of Long-Lived Assets.” ASC 360-10-15 requires us to group assets and liabilities at the lowest level for which identifiable cash flows are largely independent of the cash flows of other assets and liabilities and evaluate the asset group against the sum of the undiscounted future cash flows. If the undiscounted cash flows do not indicate the carrying amount of the asset is recoverable, an impairment charge is measured as the amount by which the carrying amount of the asset group exceeds its fair value based on discounted cash flow analysis or appraisals.
48
Goodwill acquired in a business combination is assigned to the reporting unit that is expected to benefit from the combination as of the acquisition date. Goodwill is tested for impairment on an annual basis or, more frequently, if an event occurs or circumstances change that would more likely than not reduce the fair value of the reporting unit.
Income Taxes
Income taxes are accounted for under the liability method. Deferred tax assets and liabilities are recognized for the differences between the carrying values of assets and liabilities and their respective income tax bases and for operating losses and tax credit carry forwards. A valuation allowance is provided for the portion of deferred tax assets that is more likely than not to be unrealized. Deferred tax assets and liabilities are measured using the enacted tax rates and laws.
Research and Development Costs
Research and development costs are expensed as incurred, net of related refundable investment tax credits, with the exception of non-refundable advanced payments for goods or services to be used in future research and development, which are capitalized in accordance with ASC 730, “Research and Development” and included within Prepaid Expenses or Other Assets depending on when the assets will be utilized.
Clinical trial expenses are a component of research and development costs. These expenses include fees paid to contract research organizations and investigators and other service providers, which conduct certain product development activities on our behalf. We use an accrual basis of accounting, based upon estimates of the amount of service completed. In the event payments differ from the amount of service completed, prepaid expense or accrued liabilities amounts are adjusted on the balance sheet. These expenses are based on estimates of the work performed under service agreements, milestones achieved, patient enrollment and experience with similar contracts. We monitor each of these factors to the extent possible and adjusts estimates accordingly.
Stock-Based Compensation
Effective January 1, 2006, we adopted the fair value recognition provisions of the ASC 718, “Stock Compensation”, using the modified prospective method with respect to options granted to employees and directors. Under this transition method, compensation cost is recognized in the financial statements beginning with the effective date for all share-based payments granted after January 1, 2006 and for all awards granted prior to but not yet vested as of January 1, 2006. The expense is amortized on a straight-line basis over the graded vesting period.
Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four-year period. We also granted restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision or the occurrence of other events that may have caused the awards to accelerate and vest.
Segment Information
We follow the requirements of ASC 280, “Segment Reporting.” We have one operating segment, dedicated to the development and commercialization of cytisine for smoking cessation, with operations located in Canada and the United States.
Warrants
We account for warrants pursuant to the authoritative guidance on accounting for derivative financial instruments indexed to, and potentially settled in, a company’s own stock, on the understanding that in compliance with applicable securities laws, the warrants require the issuance of registered securities upon exercise and therefore do not sufficiently preclude an implied right to net cash settlement. We classify warrants on the consolidated balance sheet as a liability which is revalued at each balance sheet date subsequent to the initial issuance. We also have warrants classified as equity and these are not reassessed for their fair value at the end of each reporting period. Warrants classified as equity are initially measured at their fair value and recognized as part of stockholders’ equity. Determining the appropriate fair-value model and calculating the fair value of registered warrants requires considerable judgment, including estimating stock price volatility and expected warrant life. The computation of expected volatility was based on the historical volatility of comparable companies from a representative peer group selected based on industry and market
49
capitalization. A small change in the estimates used may have a relatively large change in the estimated valuation. We use the Black-Scholes pricing model to value the warrants. Changes in the fair value of the warrants classified as liabilities are reflected in the consolidated statement of loss as gain (loss) on revaluation of warrants.
Reporting Currency and Foreign Currency Translation
Effective August 2, 2017, we changed the functional currency of our UK subsidiary from the Great British Pound to the U.S. dollar. As a result of the Arrangement, the UK subsidiary’s primary economic environment has now changed from the UK to the United States. This has resulted in significant changes in economic facts and circumstances that clearly indicate that the functional currency has changed. We accounted for the change in functional currency prospectively.
The consolidated financial statements for the years ended December 31, 2016 and 2015 and for the period of January 1, 2017 to August 2, 2017, are based on the UK subsidiary with a functional currency of GBP, and have been translated into the U.S. reporting currency using the current rate method as required by SFAS No. 52, “Foreign Currency Translation”, (“SFAS 52”) as follows: assets and liabilities using the rate of exchange prevailing at the balance sheet date; stockholders’ deficiency using the applicable historic rate; and revenue and expenses using the monthly average rate of exchange. Translation adjustments have been included as part of the accumulated other comprehensive income
Our functional and reporting currency is the U.S. dollar. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates.
The functional currency of our foreign subsidiary is the U.S. dollar. For this foreign operation, assets and liabilities denominated in other than U.S. dollars are translated at the period-end rates for monetary assets and liabilities and historical rates for non-monetary assets and liabilities. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates. Gains and losses from this translation are recognized in the consolidated statement of loss.
Pending Adoption of Recent Accounting Pronouncements
On February 2016, the Financial Accounting Standards Board ("FASB") issued its new leases standard, ASU No. 2016-02, Leases (Topic 842) ("ASU 2016-02"). ASU 2016-02 is aimed at putting most leases on lessees’ balance sheets, but it would also change aspects of lessor accounting. ASU 2016-02 is effective for public business entities for annual periods beginning after December 15, 2018 and interim periods within that year. This standard is expected to have a significant impact on our current accounting for our lease arrangements, particularly our current operating lease arrangements, as well as, disclosures. We are currently evaluating the impact of adoption on our financial position and results from operations.
In May 2014, the FASB, issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606): Revenue from Contracts with Customers, which guidance in this update will supersede the revenue recognition requirements in Topic 605, Revenue Recognition, and most industry-specific guidance when it becomes effective. ASU No. 2014-09 affects any entity that enters into contracts with customers to transfer goods or services or enters into contracts for the transfer of nonfinancial assets unless those contracts are within the scope of other standards. The core principal of ASU No. 2014-09 is that a company will recognize revenue when it transfers promised goods or services to customers in an amount that reflects the consideration to which the company expects to be entitled in exchange for those goods or services. In doing so, companies will need to use more judgment and make more estimates than under current guidance. These may include identifying performance obligations in the contract, estimating the amount of variable consideration to include in the transaction price and allocating the transaction price to each separate performance obligation. ASU No. 2014-09 is effective for annual reporting periods beginning after December 15, 2017, including interim periods within that reporting period, which will be our fiscal year 2018 (or December 31, 2018), and entities can transition to the standard either retrospectively or as a cumulative-effect adjustment as of the date of adoption. Early adoption is permitted. We are updating our policies and procedures to reflect the adoption of ASU No. 2014-09 and we anticipate that there is no impact on our financial statement in the year of adoption.
Recently Adopted Accounting Policies
In March 2016, the FASB issued ASU 2016-09, Improvements to Employee Share-Based Payment Accounting. ASU 2016-09 simplifies several aspects of the accounting for share-based payment transactions, including the income tax consequences, classification of awards as either equity or liabilities, and classification on the statement of cash flows. Some of the areas for simplification apply only to nonpublic entities. For public business entities, the amendments in this Update are effective for annual periods beginning after 15 December 2016, and interim periods within those annual periods. For all other entities, the amendments are effective for annual periods beginning after 15 December 2017, and interim periods within annual periods beginning after 15 December 2018. The adoption of this standard did not have a significant impact on our financial position or results of operations.
50
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes. The standard requires that deferred tax liabilities and assets be classified as noncurrent in a classified statement of financial position. Entities are currently required to separate deferred income tax liabilities and assets into current and noncurrent amounts in a classified statement of financial position. The amendments, which require non-current presentation only (by jurisdiction), are effective for financial statements issued for annual periods beginning after December 15, 2016 with earlier application permitted as of the beginning of an interim or annual reporting period. The guidance is to be applied either prospectively to all deferred tax liabilities and assets or retrospectively to all periods presented. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In February 2015, the FASB issued ASU 2015-02, Consolidation (Topic 810) — Amendments to the Consolidation Analysis. ASU 2015-02 eliminates the deferral of FAS 167 and makes changes to both the variable interest model and the voting model. For public business entities, the guidance is effective for annual and interim periods beginning after 15 December 2015. For nonpublic business entities, it is effective for annual periods beginning after 15 December 2016, and interim periods beginning after 15 December 2017. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In January 2015, the FASB issued ASU 2015-01, Income Statement—Extraordinary and Unusual Items (Subtopic 225-20): Simplifying Income Statement Presentation by Eliminating the Concept of Extraordinary Items. ASU 2015-01 eliminates the concept of reporting extraordinary items, but retains current presentation and disclosure requirements for an event or transaction that is of an unusual nature or of a type that indicates infrequency of occurrence. Transactions that meet both criteria would now also follow such presentation and disclosure requirements. For all entities, the guidance is effective for annual periods, and interim periods within those annual periods, beginning after 15 December 2015. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In August 2014, the Financial Accounting Standards Board, or FASB issued Accounting Standards Updated, or ASU No. 2014-15, Presentation of Financial Statements-Going Concern (Subtopic 2015-40) (ASU 2014-15). ASU 2014-15 provides guidance to U.S. GAAP about management’s responsibility to evaluate whether there is a substantial doubt about an entity’s ability to continue as a going concern and to provide related footnote disclosures. This new rule requires management to assess an entity’s ability to continue as a going concern by incorporating and expanding upon certain principles currently in the U.S. auditing standards. Specifically, ASU 2014-15 (1) defines the term substantial doubt, (2) requires an evaluation of every reporting period including interim periods, (3) provides principles for considering the mitigating effect of management’s plans, (5) requires an express statement and other disclosures when substantial doubt is not alleviated, and (6) requires an assessment for a period of one year after the date that the financial statements are issued (or available to be issued). This guidance is effective for annual periods ending after December 15, 2016. The adoption of this standard did not have a significant impact on our financial statement disclosures.
Interest Rate Risk
Interest rate risk is the risk that the fair values and future cash flows of financial instruments will fluctuate because of the changes in market interest rates. We invest our cash in a variety of financial instruments, primarily in short-term bank deposits, money market funds, and domestic and foreign commercial paper and government securities. These investments are denominated in U.S. dollars, and we monitor our exposure to interest rate changes is monitored. We have very limited interest rate risk due to the few assets or liabilities subject to fluctuations in interest rates. Our investment portfolio includes only marketable securities with active secondary or resale markets to help ensure portfolio liquidity. Due to the nature of our highly liquid marketable securities, a change in interest rates would not materially change the fair market value. We have estimated the effect on our portfolio of a hypothetical increase in interest rates by one percent to be a reduction of $40,000 in the fair value of our investments as of December 31, 2017.
Foreign Currency Exchange Risk
We are exposed to risks associated with foreign currency transactions on certain contracts and payroll expenses related to our Canadian subsidiary, Achieve Life Sciences Technologies Inc., denominated in Canadian dollars and our United Kingdom subsidiary, Achieve Pharma UK Limited, denominated in Great British pounds, or GBP, and we have not hedged these amounts. As our unhedged foreign currency transactions fluctuate, our earnings might be negatively affected. Accordingly, changes in the value of the U.S. dollar relative to the Canadian dollar and the GBP might have an adverse effect on our reported results of operations and financial condition, and fluctuations in exchange rates might harm our reported results and accounts from period to period. We have estimated the effect on our reported results of operations of a hypothetical increase of 10 percent in the exchange rate of the Canadian dollar and the GBP against the U.S. dollar to be $0.2 million for the year ended December 31, 2017.
51
INDEX TO FINANCIAL STATEMENTS:
52
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of Achieve Life Sciences, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Achieve Life Sciences, Inc. and its subsidiaries as of December 31, 2017 and 2016, and the related consolidated statements of loss and comprehensive loss, statements of stockholders’ equity, and statements of cash flows, for each of the three years in the period ended December 31, 2017, including the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2017 and 2016, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2017 in conformity with accounting principles generally accepted in the United States of America.
Substantial Doubt About the Company’s Ability to Continue as a Going Concern
The accompanying consolidated financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the consolidated financial statements, the Company has suffered recurring losses from operations and cash outflows from operating activities that raise substantial doubt about its ability to continue as a going concern. Management's plans in regard to these matters are also described in Note 1. The financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s consolidated financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits of these consolidated financial statements in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
PricewaterhouseCoopers LLP (signed)
Vancouver, British Columbia
March 1, 2018
We have served as the Company's auditor since 2017.
53
(In thousands, except per share and share amounts)
|
|
|
December 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
ASSETS |
|
|
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
|
|
Cash and cash equivalents [note 8] |
|
$ |
5,284 |
|
|
$ |
15 |
|
|
Restricted cash [note 8 and 14] |
|
|
222 |
|
|
|
— |
|
|
Amounts receivable |
|
|
9 |
|
|
|
— |
|
|
Prepaid expenses |
|
|
393 |
|
|
|
3 |
|
|
Total current assets |
|
|
5,908 |
|
|
|
18 |
|
|
Restricted cash [note 8] |
|
|
50 |
|
|
|
— |
|
|
Property and equipment, net [note 9] |
|
|
59 |
|
|
|
— |
|
|
Other assets [note 10] |
|
|
309 |
|
|
|
— |
|
|
License agreement [note 2, 5, 6 and 7] |
|
|
2,532 |
|
|
|
2,755 |
|
|
Goodwill [note 2 and 6] |
|
|
1,034 |
|
|
|
1,034 |
|
|
Total assets |
|
$ |
9,892 |
|
|
$ |
3,807 |
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY |
|
|
|
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
213 |
|
|
$ |
95 |
|
|
Accrued liabilities other |
|
|
438 |
|
|
|
1,121 |
|
|
Accrued clinical liabilities |
|
|
877 |
|
|
|
— |
|
|
Accrued compensation |
|
|
458 |
|
|
|
— |
|
|
Salaries Payable |
|
|
— |
|
|
|
1,028 |
|
|
Stockholder loans with related parties [note 13] |
|
|
— |
|
|
|
829 |
|
|
Current portion of long-term obligations [note 14] |
|
|
27 |
|
|
|
— |
|
|
Warrant liability [note 8 and note 12] |
|
|
— |
|
|
|
— |
|
|
Total current liabilities |
|
|
2,013 |
|
|
|
3,073 |
|
|
Deferred tax liability |
|
|
— |
|
|
|
124 |
|
|
Total liabilities |
|
|
2,013 |
|
|
|
3,197 |
|
|
Commitments and contingencies [note 14] |
|
|
|
|
|
|
|
|
|
Stockholders' equity: |
|
|
|
|
|
|
|
|
|
Common stock, $0.001 par value, 75,000,000 shares authorized, 11,956,752 and 21,230 issued at December 31, 2017 and December 31, 2016, respectively, and 11,947,932 and 21,230 outstanding at December 31, 2017 and December 31, 2016, respectively |
|
|
12 |
|
|
|
— |
|
|
Additional paid-in capital |
|
|
20,556 |
|
|
|
2,667 |
|
|
Accumulated deficit |
|
|
(12,694 |
) |
|
|
(2,062 |
) |
|
Accumulated other comprehensive income |
|
|
5 |
|
|
|
5 |
|
|
Total stockholders' equity |
|
|
7,879 |
|
|
|
610 |
|
|
Total liabilities and stockholders' equity |
|
$ |
9,892 |
|
|
$ |
3,807 |
|
|
Going concern and liquidity [note 1] |
|
|
|
|
|
|
|
|
|
Subsequent events [note 7 and note 17] |
|
|
|
|
|
|
|
|
See accompanying notes.
54
Consolidated Statements of Loss and Comprehensive Loss
(In thousands, except per share and share amounts)
|
|
|
Year Ended |
|
|
Period from 12-May-15 |
|
||||||
|
|
|
December 31, |
|
|
(inception) to |
|
||||||
|
|
|
2017 |
|
|
2016 |
|
|
31-Dec-15 |
|
|||
|
EXPENSES |
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
3,101 |
|
|
$ |
286 |
|
|
$ |
107 |
|
|
General and administrative |
|
|
3,531 |
|
|
|
1,428 |
|
|
|
1,116 |
|
|
Total operating expenses |
|
|
6,632 |
|
|
|
1,714 |
|
|
|
1,223 |
|
|
OTHER INCOME (EXPENSE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest income |
|
|
21 |
|
|
|
— |
|
|
|
— |
|
|
Bargain purchase gain [note 2] |
|
|
1,272 |
|
|
|
— |
|
|
|
— |
|
|
Contingent value rights recovery [note 2] |
|
|
200 |
|
|
|
— |
|
|
|
— |
|
|
Gain on warrants |
|
|
150 |
|
|
|
— |
|
|
|
— |
|
|
Loss on disposition of intangible asset [note 5] |
|
|
(8,610 |
) |
|
|
— |
|
|
|
— |
|
|
Other expenses |
|
|
(35 |
) |
|
|
(24 |
) |
|
|
(12 |
) |
|
Total other income |
|
|
(7,002 |
) |
|
|
(24 |
) |
|
|
(12 |
) |
|
Net loss before income taxes |
|
$ |
(13,634 |
) |
|
$ |
(1,738 |
) |
|
$ |
(1,235 |
) |
|
Recovery of deferred income taxes [note 5] |
|
|
3,051 |
|
|
|
504 |
|
|
|
407 |
|
|
Net Loss |
|
$ |
(10,583 |
) |
|
$ |
(1,234 |
) |
|
$ |
(828 |
) |
|
OTHER COMPREHENSIVE INCOME |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net unrealized gain on foreign exchange |
|
|
— |
|
|
|
4 |
|
|
|
1 |
|
|
Total other comprehensive income (loss) |
|
|
— |
|
|
|
4 |
|
|
|
1 |
|
|
Comprehensive loss |
|
$ |
(10,583 |
) |
|
$ |
(1,230 |
) |
|
$ |
(827 |
) |
|
Basic and diluted net loss per common share [note 12 [g]] |
|
$ |
(2.21 |
) |
|
$ |
(58.13 |
) |
|
$ |
(39.00 |
) |
|
Shares used in computation of basic and diluted net loss per common share [note 12 [g]] |
|
|
4,794,421 |
|
|
|
21,230 |
|
|
|
21,230 |
|
See accompanying notes.
55
Consolidated Statements of Stockholders’ Equity
(In thousands, except share amounts)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
|
Other |
|
|
|
|
|
|
Total, |
|
|||
|
|
|
Common Stock |
|
|
Paid-in |
|
|
Comprehensive |
|
|
Accumulated |
|
|
Stockholders’ |
|
|||||||||
|
|
|
Shares |
|
|
Amount |
|
|
Capital |
|
|
Income (Loss) |
|
|
Deficit |
|
|
Equity |
|
||||||
|
Balance, May 12, 2015 (date of incorporation) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Common stock issued |
|
|
11,730 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Conversion of common stock held by Extab Corporation stockholders into common stock [note 6] |
|
|
5,000 |
|
|
|
— |
|
|
|
667 |
|
|
|
— |
|
|
|
— |
|
|
|
667 |
|
|
Conversion of note payable into common stock [note 6] |
|
|
4,500 |
|
|
|
— |
|
|
|
2,000 |
|
|
|
— |
|
|
|
— |
|
|
|
2,000 |
|
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(828 |
) |
|
|
(828 |
) |
|
Other comprehensive income (loss) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
1 |
|
|
|
— |
|
|
|
1 |
|
|
Balance, December 31, 2015 |
|
|
21,230 |
|
|
|
— |
|
|
|
2,667 |
|
|
|
1 |
|
|
|
(828 |
) |
|
|
1,840 |
|
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(1,234 |
) |
|
|
(1,234 |
) |
|
Other comprehensive income (loss) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
4 |
|
|
|
— |
|
|
|
4 |
|
|
Balance, December 31, 2016 |
|
|
21,230 |
|
|
|
— |
|
|
|
2,667 |
|
|
|
5 |
|
|
|
(2,062 |
) |
|
|
610 |
|
|
Stock-based compensation expense |
|
|
— |
|
|
|
— |
|
|
|
348 |
|
|
|
— |
|
|
|
— |
|
|
|
348 |
|
|
Settlement of stockholder loans with related parties |
|
|
1,572 |
|
|
|
— |
|
|
|
2,132 |
|
|
|
— |
|
|
|
— |
|
|
|
2,132 |
|
|
Shares issued on subscription |
|
|
48 |
|
|
|
— |
|
|
|
64 |
|
|
|
— |
|
|
|
— |
|
|
|
64 |
|
|
Shares held by OncoGenex Shareholders |
|
|
2,736,709 |
|
|
|
3 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
3 |
|
|
Shares issued on conversion of Achieve common shares |
|
|
8,210,118 |
|
|
|
8 |
|
|
|
13,040 |
|
|
|
— |
|
|
|
— |
|
|
|
13,048 |
|
|
Shares cancelled on conversion of Achieve common shares |
|
|
(22,850 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Restricted Stock Unit Settlements |
|
|
5,464 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Restricted Stock Unit Settlements withheld and retired to treasury |
|
|
(1,660 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(5 |
) |
|
|
(5 |
) |
|
Shares issues - Lincoln Park Capital |
|
|
997,301 |
|
|
|
1 |
|
|
|
2,305 |
|
|
|
— |
|
|
|
— |
|
|
|
2,306 |
|
|
Purchase accounting adjustment |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(44 |
) |
|
|
(44 |
) |
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(10,583 |
) |
|
|
(10,583 |
) |
|
Balance, December 31, 2017 |
|
|
11,947,932 |
|
|
$ |
12 |
|
|
$ |
20,556 |
|
|
$ |
5 |
|
|
$ |
(12,694 |
) |
|
$ |
7,879 |
|
See accompanying notes.
56
Consolidated Statements of Cash Flows
(In thousands)
|
|
|
Year Ended |
|
|
Period from 12-May-15 |
|
||||||
|
|
|
December 31, |
|
|
(inception) to |
|
||||||
|
|
|
2017 |
|
|
2016 |
|
|
31-Dec-15 |
|
|||
|
Operating Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(10,583 |
) |
|
$ |
(1,234 |
) |
|
$ |
(828 |
) |
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gain on warrants [note 8 and note 12[e]] |
|
|
(150 |
) |
|
|
— |
|
|
|
— |
|
|
Depreciation |
|
|
59 |
|
|
|
— |
|
|
|
— |
|
|
Amortization |
|
|
223 |
|
|
|
223 |
|
|
|
140 |
|
|
Stock-based compensation [note12[c]] |
|
|
348 |
|
|
|
— |
|
|
|
— |
|
|
Deferred income tax (recovery) |
|
|
(3,051 |
) |
|
|
(504 |
) |
|
|
(407 |
) |
|
Bargain purchase gain |
|
|
(1,272 |
) |
|
|
— |
|
|
|
— |
|
|
Loss on disposition |
|
|
8,610 |
|
|
|
— |
|
|
|
— |
|
|
Contingent value rights recovery |
|
|
(200 |
) |
|
|
— |
|
|
|
— |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Amounts receivable |
|
|
(9 |
) |
|
|
— |
|
|
|
— |
|
|
Prepaid expenses and other assets |
|
|
(1,349 |
) |
|
|
(2 |
) |
|
|
— |
|
|
Accounts payable |
|
|
118 |
|
|
|
22 |
|
|
|
57 |
|
|
Accrued liabilities other |
|
|
(2,185 |
) |
|
|
670 |
|
|
|
284 |
|
|
Accrued clinical liabilities |
|
|
877 |
|
|
|
— |
|
|
|
— |
|
|
Accrued compensation |
|
|
458 |
|
|
|
— |
|
|
|
— |
|
|
Salaries payable |
|
|
(1,028 |
) |
|
|
623 |
|
|
|
404 |
|
|
Lease obligation |
|
|
27 |
|
|
|
— |
|
|
|
— |
|
|
Net cash used in operating activities |
|
|
(9,107 |
) |
|
|
(202 |
) |
|
|
(350 |
) |
|
Financing Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Proceeds from share subscription |
|
|
64 |
|
|
|
— |
|
|
|
— |
|
|
Proceeds from ATM Financing, net of issuance costs |
|
|
1,942 |
|
|
|
— |
|
|
|
— |
|
|
Taxes paid related to net share settlement of equity awards |
|
|
(5 |
) |
|
|
— |
|
|
|
— |
|
|
Payments on loan |
|
|
— |
|
|
|
— |
|
|
|
(272 |
) |
|
Stockholder loans |
|
|
— |
|
|
|
150 |
|
|
|
2,683 |
|
|
Net cash provided by financing activities |
|
|
2,001 |
|
|
|
150 |
|
|
|
2,411 |
|
|
Investing Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash received on reverse takeover of OncoGenex |
|
|
12,648 |
|
|
|
— |
|
|
|
— |
|
|
Purchase of Extab Corporation common stock [note 6] |
|
|
— |
|
|
|
— |
|
|
|
(2,000 |
) |
|
Net cash provided by (used in) investing activities |
|
|
12,648 |
|
|
|
— |
|
|
|
(2,000 |
) |
|
Effect of exchange rate changes on cash |
|
|
(1 |
) |
|
|
— |
|
|
|
— |
|
|
Net increase (decrease) in cash, cash equivalents and restricted cash |
|
|
5,541 |
|
|
|
(52 |
) |
|
|
61 |
|
|
Cash, cash equivalents and restricted cash at beginning of year |
|
|
15 |
|
|
|
67 |
|
|
|
6 |
|
|
Cash, cash equivalents and restricted cash at end of year |
|
$ |
5,556 |
|
|
$ |
15 |
|
|
$ |
67 |
|
|
Supplemental Disclosure of Cash Flow Information: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense accrued but not yet paid |
|
$ |
— |
|
|
$ |
26 |
|
|
$ |
11 |
|
See accompanying notes.
57
Notes to Consolidated Financial Statements
(In thousands, except per share and share amounts)
1. NATURE OF BUSINESS AND BASIS OF PRESENTATION
Achieve Life Sciences, Inc. (referred to as “Achieve,” “we,” “us,” or “our”) is a clinical-stage pharmaceutical company committed to the global development and commercialization of cytisine for smoking cessation. We were incorporated in the state of Delaware, and operate out of Vancouver, British Columbia and Bothell, Washington.
On August 1, 2017, OncoGenex Pharmaceuticals, Inc., or OncoGenex, completed a transaction, or the Arrangement, with Achieve Life Science, Inc., or Achieve, as contemplated by the Merger Agreement between Achieve and OncoGenex dated January 5, 2017, or the Merger Agreement. Under the terms of the Merger Agreement, OncoGenex changed its name to Achieve Life Sciences, Inc., instituted an one-for-eleven reverse stock split, issued 8,210,118 shares of its common stock (after accounting for the elimination of resulting fractional shares) in exchange for all of the outstanding preferred shares, common shares and convertible debentures of Achieve, as a result Achieve became a wholly-owned subsidiary of OncoGenex, and is listed on the Nasdaq Capital Market under the ticker symbol ACHV.
These consolidated financial statements account for the Arrangement between OncoGenex and Achieve as a reverse merger, whereby Achieve is deemed to be the acquiring entity from an accounting perspective. The consolidated results of operations of the Company for the year ended December 31, 2017 include the results of operations of only Achieve for the time period of January 1, 2017 through August 1, 2017 and include the results of the combined company following the completion of the Arrangement on August 1, 2017. The consolidated results of operations for the years ended December 31, 2016 and December 31, 2015 include only the consolidated results of operations of Achieve and do not include historical results of OncoGenex. This treatment and presentation is in accordance with ASC 805, “Business Combinations”. Information relating to the number of shares, price per share and per share amounts of common stock are presented on a post- reverse stock split basis, as a reverse stock split in the ratio of one-for-eleven was effected in connection with the Arrangement. The accompanying consolidated Balance Sheet at December 31, 2016 has been derived from the audited consolidated financial statements included in our Amendment No. 3 to the Registration Statement on Form S-4/A filed with the Securities and Exchange Commission, or SEC, on June 6, 2017. Accordingly, these financial statements should be read in conjunction with the audited consolidated financial statements and the related notes thereto included in the Amendment No. 3 to the Registration Statement on Form S-4/A filed with the SEC on June 6, 2017.
Basis of Presentation
The consolidated financial statements include the accounts of Achieve and our wholly owned subsidiaries, Achieve Life Sciences Technologies Inc., Achieve Life Science, Inc., Extab Corporation, and Achieve Pharma UK Limited. All intercompany balances and transactions have been eliminated.
Liquidity
We have historically experienced recurring losses from operations that have generated an accumulated deficit of $12.7 million through December 31, 2017. For the year ended December 31, 2017, we incurred a net loss of $10.6 million. As of December 31, 2017, we had a cash and cash equivalents balance of $5.3 million and a positive working capital balance of $3.7 million.
The accompanying financial statements have been prepared assuming we will continue to operate as a going concern, which contemplates the realization of assets and liabilities and commitments in the normal course of business.
Substantial doubt exists as to our ability to continue as a going concern. Our ability to continue as a going concern is uncertain and dependent on our ability to obtain additional financing. There is no assurance that we will obtain additional financing from other sources. We have, thus far, financed our operations through the closing of the Arrangement (Note 2—Reverse Merger) and equity financing (Note 12—Common Stock). Without additional funds, we may be forced to delay, scale back or eliminate some of our research and development activities or other operations and potentially delay product development in an effort to provide sufficient funds to continue our operations. If any of these events occurs, our ability to achieve our development and commercialization goals would be adversely affected.
Our current capital resources are insufficient to fund our planned operations for the next 12 months. We will continue to require substantial additional capital to continue our clinical development activities. Accordingly, we will need to raise substantial additional capital to continue to fund our operations from the sale of our securities, partnering arrangements or other financing transactions in order to finance the commercialization of our product candidates. The amount and timing of our future funding requirements will
58
depend on many factors, including the pace and results of our clinical development efforts. Failure to raise capital as and when needed, on favorable terms or at all, will have a negative impact on our financial condition and our ability to develop our product candidate. We expect our research and development expenses to substantially increase in connection with our ongoing activities, particularly as we advance our product candidate in clinical development.
The consolidated financial statements do not include any adjustments to the amounts and classification of assets and liabilities that might be necessary should we be unable to continue as a going concern. Such adjustments could be material.
2. REVERSE MERGER
The consolidated financial statements account for the Arrangement between us and OncoGenex, whereby OncoGenex acquired all of our outstanding common shares, as a reverse merger wherein we are deemed to be the acquiring entity from an accounting perspective. The consolidated results of operations include our results of operations for the twelve months ended December 31, 2017 and the results of OncoGenex following the completion of the Arrangement on August 1, 2017. The consolidated results of operations for twelve months ended December 31, 2016 include only our consolidated results of operations and do not include historical results of OncoGenex.
On August 1, 2017, our stockholders approved the Arrangement described above and on the same date, OncoGenex stockholders approved the Arrangement and a one-for-eleven reverse stock split of its common stock. The reverse stock split occurred immediately prior to the closing of the Arrangement. Resulting fractional shares were eliminated. All information in the financial statements and the notes thereto relating to the number of shares, price per share, and per share amounts of common stock are presented on a post-split basis.
Under the purchase method of accounting, OncoGenex’s outstanding shares of common stock were valued using the closing price on NASDAQ of $4.62 as at August 1, 2017. There were 2,736,703 shares of common stock outstanding, as adjusted for the reverse stock split, on August 1, 2017, immediately prior to closing. The fair value of the OncoGenex outstanding stock options was determined using the Black-Scholes pricing model with the following assumptions: stock price of $4.62, volatility of 97.23% to 106.63%, risk-free interest rate of 1.31% to 1.54%, and expected lives ranging from 1.82 to 3.31 years. The fair value of the OncoGenex outstanding warrants was determined using the Black-Scholes pricing model with the following assumptions: stock price of $4.62, volatility of 90.33% to 106.08%, risk-free interest rate of 1.32% to 1.53%, and expected lives ranging from 1.91 to 3.24 years.
The final purchase price is summarized as follows (dollars in thousands, except per share amounts):
|
Shares of the combined company to be owned by OncoGenex equity holders |
|
|
2,736,709 |
|
|
Multiplied by the price per share of OncoGenex stock |
|
$ |
4.62 |
|
|
Value of shares of the combined company owned by OncoGenex equity holders |
|
$ |
12,643 |
|
|
Fair value of options and warrants assumed |
|
$ |
207 |
|
|
Fair value of contingent value rights assumed |
|
$ |
200 |
|
|
Total purchase price |
|
$ |
13,050 |
|
Under the purchase method of accounting, the total purchase price as shown in the table above is allocated to the OncoGenex net tangible and identifiable intangible assets acquired and liabilities assumed based on their fair values as of the date of the completion of the Arrangement. The final purchase price allocation is as follows (in thousands):
|
Cash, cash equivalents and marketable securities |
|
$ |
12,376 |
|
|
Prepaid expenses and other assets |
|
|
518 |
|
|
Intangible assets license agreements |
|
|
8,610 |
|
|
Accounts payable, accrued expenses and other liabilities |
|
|
(4,054 |
) |
|
Deferred tax liability |
|
|
(2,928 |
) |
|
Contingent value rights |
|
|
(200 |
) |
|
Excess negative goodwill |
|
|
(1,272 |
) |
|
Total purchase price |
|
|
13,050 |
|
In accordance with ASC 805, “Business Combinations,” any excess of fair value of acquired net assets over purchase price (negative goodwill) has been recognized as a gain in the period the Arrangement was completed. We have reassessed whether all acquired assets and assumed liabilities have been identified and recognized and performed remeasurements to verify that the consideration paid, assets acquired, and liabilities assumed have been properly valued. The remaining excess has been recognized as a gain. There was no other impact to other comprehensive income.
59
OncoGenex issued contingent value rights, or each, a CVR and collectively, the CVRs, on July 31, 2017 to their existing stockholders as of July 27, 2017. One CVR was issued for each share of their common stock outstanding as of the record date for such issuance. Each CVR was a non-transferable right to potentially receive certain cash, equity or other consideration received by us in the event that we received any such consideration during the five-year period after consummation of the Arrangement as a result of the achievement of certain clinical milestones, regulatory milestones, sales-based milestones and/or up-front payment milestones relating to apatorsen, or the Milestones, upon the terms and subject to the conditions set forth in a contingent value rights agreement to be entered into between us and an as of yet unidentified third party, as rights agent, or the CVR Agreement. The aggregate consideration to be distributed to the holders of the CVRs would have been equal to 80% of the consideration received by us as a result of the achievement of the Milestones less certain agreed to offsets, as determined pursuant to the CVR Agreement.
The contingent value rights expired on August 17, 2017, as we did not enter into any term sheets or agreement with third parties for the development or commercialization of apatorsen. A recovery of $0.2 million was recognized on our Consolidated Statements of Loss and Comprehensive Loss.
Pro Forma Results of Operations
The results of operations of OncoGenex are included in our consolidated financial statements following the date of the completion of the transaction on August 1, 2017. The following table presents pro forma results of operations and gives effect to the business combination transaction as if the transaction was consummated at the beginning of the period presented. The unaudited pro forma results of operations are not necessarily indicative of what would have occurred had the business combination been completed at the beginning of the retrospective periods or of the results that may occur in the future.
|
|
|
For the year ended |
|
|
For the year ended |
|
||
|
|
|
December 31, |
|
|
December 31, |
|
||
|
|
|
2017 |
|
|
2016 |
|
||
|
|
|
(Unaudited) |
|
|
(Unaudited) |
|
||
|
Revenue |
|
$ |
— |
|
|
$ |
5,062 |
|
|
Net loss applicable to common shareholders |
|
$ |
(20,111 |
) |
|
$ |
(21,363 |
) |
|
Net loss per share-basic and diluted |
|
$ |
(4.19 |
) |
|
$ |
(7.79 |
) |
|
Weighted average shares |
|
|
4,794,421 |
|
|
|
2,743,906 |
|
3. ACCOUNTING POLICIES
Significant Accounting Policies
Use of Estimates
The preparation of consolidated financial statements in conformity with United States generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and notes thereto. Actual results could differ from these estimates. Estimates and assumptions principally relate to estimates of the fair value of our warrant liability, the initial fair value and forfeiture rates of stock options issued to employees and consultants, the estimated compensation cost on performance restricted stock unit awards and clinical trial and manufacturing accruals, estimated useful lives of property, plant and equipment and estimates and assumptions in contingent liabilities.
Cash Equivalents
We consider all highly liquid investments with an original maturity of three months or less to be cash equivalents, which we consider as available for sale and carry at fair value, with unrealized gains and losses, if any, reported as accumulated other comprehensive income or loss, which is a separate component of stockholders’ equity.
Short-Term Investments
Short-term investments consist of financial instruments purchased with an original maturity of greater than three months and less than one year. We consider our short-term investments as available-for-sale and carry them at fair value, with unrealized gains and losses except other than temporary losses, if any, reported as accumulated other comprehensive income or loss, which is a separate
60
component of stockholders’ equity. Realized gains and losses on the sale of these securities are recognized in net income or loss. The cost of investments sold is based on the specific identification method.
Fair value of financial instruments
The fair value of our cash equivalents and marketable securities is based on quoted market prices and trade data for comparable securities. We determine the fair value of our warrant liability based on the Black-Scholes pricing model and using considerable judgment, including estimating stock price volatility and expected warrant life. Other financial instruments including amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities and accrued compensation are carried at cost, which we believe approximates fair value because of the short-term maturities of these instruments.
Intellectual Property
The costs of acquiring intellectual property rights to be used in the research and development process, including licensing fees and milestone payments, are charged to research and development expense as incurred in situations where we have not identified an alternative future use for the acquired rights, and are capitalized in situations where we have identified an alternative future use. No costs associated with acquiring intellectual property rights have been capitalized to date. Costs of maintaining intellectual property rights are expensed as incurred.
Intangible Assets
Our intangible assets are subject to amortization and are amortized using the straight-line method over their estimated period of benefit. We evaluate the carrying amount of intangible assets periodically by taking into account events or circumstances that may warrant revised estimates of useful lives or that indicate the asset may be impaired.
Goodwill
Goodwill acquired in a business combination is assigned to the reporting unit that is expected to benefit from the combination as of the acquisition date. Goodwill is tested for impairment on an annual basis or, more frequently, if an event occurs or circumstances change that would more likely than not reduce the fair value of the reporting unit.
Property and Equipment
Property and equipment assets are recorded at cost less accumulated depreciation. Depreciation expense on assets acquired under capital lease is recorded within depreciation expense. Depreciation is recorded on a straight-line basis over the following periods:
|
Computer equipment |
|
3 years |
|
Furniture and fixtures |
|
5 years |
|
Machinery and equipment |
|
5 - 10 years |
|
Leasehold improvements and equipment under capital lease |
|
Over the term of the lease |
Impairment of Long-Lived Assets
We review long-lived assets for impairment whenever events or changes in circumstances indicate that the asset’s carrying amount may not be recoverable. We conduct our long-lived asset impairment analyses in accordance with ASC 360-10-15, “Impairment or Disposal of Long-Lived Assets.” ASC 360-10-15 requires us to group assets and liabilities at the lowest level for which identifiable cash flows are largely independent of the cash flows of other assets and liabilities and evaluate the asset group against the sum of the undiscounted future cash flows. If the undiscounted cash flows do not indicate the carrying amount of the asset is recoverable, an impairment charge is measured as the amount by which the carrying amount of the asset group exceeds its fair value based on discounted cash flow analysis or appraisals.
Income Taxes
Income taxes are accounted for under the liability method. Deferred tax assets and liabilities are recognized for the differences between the carrying values of assets and liabilities and their respective income tax bases and for operating losses and tax credit carry forwards. A valuation allowance is provided for the portion of deferred tax assets that is more likely than not to be unrealized. Deferred tax assets and liabilities are measured using the enacted tax rates and laws.
61
Research and Development Costs
Research and development costs are expensed as incurred, net of related refundable investment tax credits, with the exception of non-refundable advanced payments for goods or services to be used in future research and development, which are capitalized in accordance with ASC 730, “Research and Development” and included within Prepaid Expenses or Other Assets depending on when the assets will be utilized.
Clinical trial expenses are a component of research and development costs. These expenses include fees paid to contract research organizations and investigators and other service providers, which conduct certain product development activities on our behalf. We use an accrual basis of accounting, based upon estimates of the amount of service completed. In the event payments differ from the amount of service completed, prepaid expense or accrued liabilities amounts are adjusted on the balance sheet. These expenses are based on estimates of the work performed under service agreements, milestones achieved, patient enrollment and experience with similar contracts. We monitor each of these factors to the extent possible and adjusts estimates accordingly.
Stock-Based Compensation
Effective January 1, 2006, we adopted the fair value recognition provisions of the ASC 718, “Stock Compensation”, using the modified prospective method with respect to options granted to employees and directors. Under this transition method, compensation cost is recognized in the financial statements beginning with the effective date for all share-based payments granted after January 1, 2006 and for all awards granted prior to but not yet vested as of January 1, 2006. The expense is amortized on a straight-line basis over the graded vesting period.
Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four-year period. We also granted restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision or the occurrence of other events that may have caused the awards to accelerate and vest.
Segment Information
We follow the requirements of ASC 280, “Segment Reporting.” We have one operating segment, dedicated to the development and commercialization of cytisine for smoking cessation, with operations located in Canada and the United States.
Comprehensive Income (Loss)
Comprehensive income (loss) is comprised of net income (loss) and other comprehensive income (loss). Other comprehensive income (loss) consists of unrealized gains and losses on our available-for-sale marketable securities. We report the components of comprehensive loss in the statement of stockholders’ equity.
Loss per Common Share
Basic loss per common share is computed using the weighted average number of common shares outstanding during the period. Diluted loss per common share is computed in accordance with the treasury stock method. The effect of potentially issuable common shares from outstanding stock options, restricted stock unit awards and warrants are anti-dilutive for all periods presented.
Warrants
We account for warrants pursuant to the authoritative guidance on accounting for derivative financial instruments indexed to, and potentially settled in, a company’s own stock, on the understanding that in compliance with applicable securities laws, the warrants require the issuance of registered securities upon exercise and therefore do not sufficiently preclude an implied right to net cash settlement. We classify warrants on the consolidated balance sheet as a liability which is revalued at each balance sheet date subsequent to the initial issuance. We also have warrants classified as equity and these are not reassessed for their fair value at the end of each reporting period. Warrants classified as equity are initially measured at their fair value and recognized as part of stockholders’ equity. Determining the appropriate fair-value model and calculating the fair value of registered warrants requires considerable judgment, including estimating stock price volatility and expected warrant life. The computation of expected volatility was based on the historical volatility of comparable companies from a representative peer group selected based on industry and market capitalization. A small change in the estimates used may have a relatively large change in the estimated valuation. We use the Black-
62
Scholes pricing model to value the warrants. Changes in the fair value of the warrants classified as liabilities are reflected in the consolidated statement of loss as gain (loss) on revaluation of warrants.
Reporting Currency and Foreign Currency Translation
Effective August 2, 2017, we changed the functional currency of our UK subsidiary from the Great British Pound to the U.S. dollar. As a result of the Arrangement, the UK subsidiary’s primary economic environment has now changed from the UK to the United States. This has resulted in significant changes in economic facts and circumstances that clearly indicate that the functional currency has changed. We accounted for the change in functional currency prospectively.
The consolidated financial statements for the years ended December 31, 2016 and 2015 and for the period of January 1, 2017 to August 2, 2017, are based on the UK subsidiary with a functional currency of GBP, and have been translated into the U.S. reporting currency using the current rate method as required by SFAS No. 52, “Foreign Currency Translation”, (“SFAS 52”) as follows: assets and liabilities using the rate of exchange prevailing at the balance sheet date; stockholders’ deficiency using the applicable historic rate; and revenue and expenses using the monthly average rate of exchange. Translation adjustments have been included as part of the accumulated other comprehensive income
Our functional and reporting currency is the U.S. dollar. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates.
The functional currency of our foreign subsidiary is the U.S. dollar. For this foreign operation, assets and liabilities denominated in other than U.S. dollars are translated at the period-end rates for monetary assets and liabilities and historical rates for non-monetary assets and liabilities. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates. Gains and losses from this translation are recognized in the consolidated statement of loss.
Pending Adoption of Recent Accounting Pronouncements
On February 2016, the Financial Accounting Standards Board ("FASB") issued its new leases standard, ASU No. 2016-02, Leases (Topic 842) ("ASU 2016-02"). ASU 2016-02 is aimed at putting most leases on lessees’ balance sheets, but it would also change aspects of lessor accounting. ASU 2016-02 is effective for public business entities for annual periods beginning after December 15, 2018 and interim periods within that year. This standard is expected to have a significant impact on our current accounting for our lease arrangements, particularly our current operating lease arrangements, as well as, disclosures. We are currently evaluating the impact of adoption on our financial position and results from operations.
In May 2014, the FASB, issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606): Revenue from Contracts with Customers, which guidance in this update will supersede the revenue recognition requirements in Topic 605, Revenue Recognition, and most industry-specific guidance when it becomes effective. ASU No. 2014-09 affects any entity that enters into contracts with customers to transfer goods or services or enters into contracts for the transfer of nonfinancial assets unless those contracts are within the scope of other standards. The core principal of ASU No. 2014-09 is that a company will recognize revenue when it transfers promised goods or services to customers in an amount that reflects the consideration to which the company expects to be entitled in exchange for those goods or services. In doing so, companies will need to use more judgment and make more estimates than under current guidance. These may include identifying performance obligations in the contract, estimating the amount of variable consideration to include in the transaction price and allocating the transaction price to each separate performance obligation. ASU No. 2014-09 is effective for annual reporting periods beginning after December 15, 2017, including interim periods within that reporting period, which will be our fiscal year 2018 (or December 31, 2018), and entities can transition to the standard either retrospectively or as a cumulative-effect adjustment as of the date of adoption. Early adoption is permitted. We are updating our policies and procedures to reflect the adoption of ASU No. 2014-09 and we anticipate that there is no impact on our financial statement in the year of adoption.
Recently Adopted Accounting Policies
In March 2016, the FASB issued ASU 2016-09, Improvements to Employee Share-Based Payment Accounting. ASU 2016-09 simplifies several aspects of the accounting for share-based payment transactions, including the income tax consequences, classification of awards as either equity or liabilities, and classification on the statement of cash flows. Some of the areas for simplification apply only to nonpublic entities. For public business entities, the amendments in this Update are effective for annual periods beginning after 15 December 2016, and interim periods within those annual periods. For all other entities, the amendments are effective for annual periods beginning after 15 December 2017, and interim periods within annual periods beginning after 15 December 2018. The adoption of this standard did not have a significant impact on our financial position or results of operations.
63
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes. The standard requires that deferred tax liabilities and assets be classified as noncurrent in a classified statement of financial position. Entities are currently required to separate deferred income tax liabilities and assets into current and noncurrent amounts in a classified statement of financial position. The amendments, which require non-current presentation only (by jurisdiction), are effective for financial statements issued for annual periods beginning after December 15, 2016 with earlier application permitted as of the beginning of an interim or annual reporting period. The guidance is to be applied either prospectively to all deferred tax liabilities and assets or retrospectively to all periods presented. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In February 2015, the FASB issued ASU 2015-02, Consolidation (Topic 810) — Amendments to the Consolidation Analysis. ASU 2015-02 eliminates the deferral of FAS 167 and makes changes to both the variable interest model and the voting model. For public business entities, the guidance is effective for annual and interim periods beginning after 15 December 2015. For nonpublic business entities, it is effective for annual periods beginning after 15 December 2016, and interim periods beginning after 15 December 2017. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In January 2015, the FASB issued ASU 2015-01, Income Statement—Extraordinary and Unusual Items (Subtopic 225-20): Simplifying Income Statement Presentation by Eliminating the Concept of Extraordinary Items. ASU 2015-01 eliminates the concept of reporting extraordinary items, but retains current presentation and disclosure requirements for an event or transaction that is of an unusual nature or of a type that indicates infrequency of occurrence. Transactions that meet both criteria would now also follow such presentation and disclosure requirements. For all entities, the guidance is effective for annual periods, and interim periods within those annual periods, beginning after 15 December 2015. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In August 2014, the Financial Accounting Standards Board, or FASB issued Accounting Standards Updated, or ASU No. 2014-15, Presentation of Financial Statements-Going Concern (Subtopic 2015-40) (ASU 2014-15). ASU 2014-15 provides guidance to U.S. GAAP about management’s responsibility to evaluate whether there is a substantial doubt about an entity’s ability to continue as a going concern and to provide related footnote disclosures. This new rule requires management to assess an entity’s ability to continue as a going concern by incorporating and expanding upon certain principles currently in the U.S. auditing standards. Specifically, ASU 2014-15 (1) defines the term substantial doubt, (2) requires an evaluation of every reporting period including interim periods, (3) provides principles for considering the mitigating effect of management’s plans, (5) requires an express statement and other disclosures when substantial doubt is not alleviated, and (6) requires an assessment for a period of one year after the date that the financial statements are issued (or available to be issued). This guidance is effective for annual periods ending after December 15, 2016. The adoption of this standard did not have a significant impact on our financial statement disclosures.
4. FINANCIAL INSTRUMENTS AND RISK
For certain of our financial instruments, including cash and cash equivalents, amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities and accrued compensation carrying values approximate fair value due to their short-term nature. Our cash equivalents and short-term investments are recorded at fair value.
Financial risk is the risk to our results of operations that arises from fluctuations in interest rates and foreign exchange rates and the degree of volatility of these rates as well as credit risk associated with the financial stability of the issuers of the financial instruments. Foreign exchange rate risk arises as a portion of our investments which finance operations and a portion of our expenses are denominated in other than U.S. dollars.
We invest our excess cash in accordance with investment guidelines, which limit our credit exposure to any one financial institution or corporation other than securities issued by the U.S. government. We only invest in A (or equivalent) rated securities with maturities of one year or less. These securities generally mature within one year or less and in some cases are not collateralized. At December 31, 2017 the average days to maturity of our portfolio of cash equivalents and marketable securities was zero days. We do not use derivative instruments to hedge against any of these financial risks.
5. INTANGIBLES
All of our intangible assets are subject to amortization and are amortized using the straight-line method over their estimated useful life.
We acquired license agreements, related to OncoGenex’s product candidate apatorsen, upon the acquisition of OncoGenex. As at the date of the acquisition, the agreements were determined to have a fair value of $8.6 million with an estimated useful life of 6 years. (Note 2—Reverse Merger)
64
In August 2017, we discontinued further development of apatorsen. We provided a notice of discontinuance to our former development partners for apatorsen, Ionis Pharmaceuticals, Inc., or Ionis, and a letter of termination to the University of British Columbia, or UBC, notifying them that we have discontinued development of apatorsen resulting in termination of all licensing agreements related to this product candidate. We believe that all financial obligations, other than continuing mutual indemnification obligations and our requirement to pay for out-of-pocket patent expenses incurred up to the date of termination and for abandoning the apatorsen patents and patent applications, under all apatorsen related agreements with Ionis and UBC, are no longer owed and no further payments are due. We recognized a loss on disposition of apatorsen of $8.6 million and a deferred income tax recovery of $2.9 million as a result of discontinuing the development program and providing a notice of discontinuance of the license agreements with Ionis.
We acquired license and supply agreements, in relation to cytisine, upon the acquisition of Extab Corporation, or Extab. The agreements were determined to have a fair value of $3.1 million with an estimated useful life of 14 years (Note 6— Extab Acquisition).
The components of intangible assets were as follows:
|
|
|
December 31, 2017 |
|
|
December 31, 2016 |
|
||||||||||||||||||
|
|
|
Gross Carrying |
|
|
Accumulated |
|
|
Net Carrying |
|
|
Gross Carrying |
|
|
Accumulated |
|
|
Net Carrying |
|
||||||
|
|
|
Value |
|
|
Amortization |
|
|
Value |
|
|
Value |
|
|
Amortization |
|
|
Value |
|
||||||
|
License Agreements |
|
$ |
3,117 |
|
|
$ |
(585 |
) |
|
$ |
2,532 |
|
|
$ |
3,117 |
|
|
$ |
(362 |
) |
|
$ |
2,755 |
|
For the year ended December 31, 2017 and 2016 we recorded license agreement amortization expense of $0.2 million and $0.2 million, respectively. The following table outlines the estimated future amortization expense related to intangible assets held as of December 31, 2017:
|
Year Ending December 31, |
|
|
|
|
|
2018 |
|
|
223 |
|
|
2019 |
|
|
223 |
|
|
2020 |
|
|
223 |
|
|
2021 |
|
|
223 |
|
|
Thereafter |
|
|
1,640 |
|
|
Total |
|
$ |
2,532 |
|
We evaluate the carrying amount of intangible assets periodically by taking into account events or circumstances that may warrant revised estimates of useful life or that indicate the asset may be impaired. We conducted an impairment analysis for long lived assets, including the license and supply agreements for the active pharmaceutical ingredient cytisine, and concluded no impairment has occurred as of December 31, 2017.
6. EXTAB ACQUISITION
On May 14, 2015, we entered into a Share Purchase Agreement with Sopharma, AD, or Sopharma, a public pharmaceutical company located in Bulgaria, to acquire 75% of the outstanding shares of Extab.
Pursuant to the Share Purchase Agreement, we acquired a 75% controlling interest in Extab from Sopharma for $2.0 million in cash and $2.0 million in a deferred payment, contingent on regulatory approval of cytisine by the Food and Drug Administration, or FDA, or the European Medicines Agency, or EMA. In addition, as part of and in conjunction with the Share Purchase Agreement, we amended our existing license and supply agreements with Sopharma, extending their terms by five years and reducing the royalty rate payable by us. (Note 7—License Agreements) Subsequent to the acquisition, we paid to Sopharma $0.3 million to retire the balance of Extab’s outstanding loans with Sopharma.
The acquisition was accounted for using the acquisition method under ASC 805 business combinations. Results of operations have been included in the financial statements from the date of acquisition May 18, 2015, the date we assumed control of Extab. The fair value of the business combination was determined using level 3 inputs.
65
The purchase price of our 75% controlling interest in Extab was as follows:
|
Cash consideration |
|
$ |
2,000 |
|
|
Contingent consideration |
|
|
— |
|
|
Purchase Price |
|
$ |
2,000 |
|
As of the date of acquisition we assessed the likelihood of meeting the contingent event as unlikely and as a result have estimated its fair value at zero. We consider the best indicator of the fair value of net assets acquired to be the $2.0 million cash consideration paid to acquire our 75% controlling interest plus the $0.7 million fair value attributable to the non-controlling interest, or NCI, calculated on a proportionate basis.
Under the acquisition method of accounting, the total purchase price is allocated to the acquired tangible and intangible assets and assumed liabilities of Extab based on their estimated fair values as of the transaction closing date. The allocation of the purchase price based on the estimated fair values is as follows:
|
|
|
Fair Value |
|
|
|
Cash |
|
$ |
6 |
|
|
License agreements |
|
$ |
3,117 |
|
|
Goodwill |
|
$ |
1,034 |
|
|
Other current liabilities |
|
$ |
(456 |
) |
|
Deferred tax liability |
|
$ |
(1,034 |
) |
|
Non-controlling interest |
|
$ |
(667 |
) |
|
|
|
$ |
2,000 |
|
The license agreement expires May 26, 2029. As of the acquisition date, we estimated its useful life to be the same as the remaining 14 year contractual life. We also elected to amortize intangible assets on a straight line basis over its useful life, since there is no pattern of successful economic benefits available at the time to reliably determine a different amortization.
Subsequent to acquiring control of Extab, we entered into an agreement with the NCI stockholder of Extab to convert their shares in Extab into shares of our common stock. As of September 30, 2015, all of the NCI had converted their shares in Extab into shares of our common stock resulting in elimination of the Extab non-controlling interest and Extab becoming a wholly-owned subsidiary of us.
7. LICENSE AGREEMENTS
Sopharma License and Supply Agreements
In 2009 and 2010, we entered into a license agreement, or the Sopharma License Agreement, and a supply agreement, or the Sopharma Supply Agreement, with Sopharma, AD, or Sopharma. Pursuant to the Sopharma License Agreement, we were granted access to all available manufacturing, efficacy and safety data related to cytisine, as well as a granted patent in several European countries including Germany, France and Italy related to new oral dosage forms of cytisine providing enhanced stability. Additional rights granted under the Sopharma License Agreement include the exclusive use of, and the right to sublicense, the trademark Tabex in all territories—other than certain countries in Central and Eastern Europe, Scandinavia, North Africa, the Middle East and Central Asia, as well as Vietnam, where Sopharma or its affiliates and agents already market Tabex—in connection with the marketing, distribution and sale of products. Under the Sopharma License Agreement, we agreed to pay a nonrefundable license fee. In addition, we agreed to make certain royalty payments equal to a mid-teens percentage of all net sales of Tabex branded products in our territory during the term of the Sopharma License Agreement, including those sold by a third party pursuant to any sublicense which may be granted by us. We have agreed to cooperate with Sopharma in the defense against any actual or threatened infringement claims with respect to Tabex. Sopharma has the right to terminate the Sopharma License Agreement upon the termination or expiration of the Sopharma Supply Agreement. The Sopharma License Agreement will also terminate under customary termination provisions including bankruptcy or insolvency and material breach. To date, we have paid Sopharma $10 pursuant to the Sopharma License Agreement.
A cross-license exists between us and Sopharma whereby we grant to Sopharma rights to any patents or patent applications or other intellectual property rights filed by us in Sopharma territories.
66
On May 14, 2015, we and Sopharma entered into an amendment to the Sopharma License Agreement. Among other things, the amendment to the Sopharma License Agreement reduced the royalty payments payable by us to Sopharma from a percentage in the mid-teens to a percentage in the mid-single digits and extended the term of the Sopharma License Agreement until May 26, 2029.
On July 28, 2017, we and Sopharma entered into the amended and restated Sopharma Supply Agreement. Pursuant to the amended and restated Sopharma Supply Agreement, for territories as detailed in the licensing agreement, we will exclusively purchase all of our cytisine from Sopharma, and Sopharma agrees to exclusively supply all such cytisine requested by us, and we extended the term to 2037. In addition, we will have full access to the cytisine supply chain and Sopharma will manufacture sufficient cytisine to meet a forecast for a specified demand of cytisine for the five years commencing shortly after the commencement of the agreement, with the forecast to be updated regularly thereafter. Each of us and Sopharma may terminate the Sopharma Supply Agreement in the event of the other party’s material breach or bankruptcy or insolvency.
University of Bristol License Agreement
In July 2016, we entered into a license agreement with the University of Bristol, or the University of Bristol License Agreement. Under the University of Bristol License Agreement, we received exclusive and nonexclusive licenses from the University of Bristol to certain patent and technology rights resulting from research activities into cytisine and its derivatives for use in smoking cessation, including a number of patent applications related to novel approaches to cytisine binding at the nicotinic receptor level. Any patents issued in connection with these applications would be scheduled to expire on February 5, 2036 at the earliest.
In consideration of rights granted by the University of Bristol, we agreed to pay amounts of up to $3.2 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the University of Bristol License Agreement. Additionally, if we successfully commercialize product candidates subject to the University of Bristol License Agreement, we are responsible for royalty payments in the low-single digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products.
On January 22, 2018, we and the University of Bristol entered into an amendment to the University of Bristol License Agreement. Pursuant to the amended University of Bristol License Agreement we received exclusive rights for all human medicinal uses of cytisine across all therapeutic categories from the University of Bristol from research activities into cytisine and its derivatives. In consideration of rights granted by the amended University of Bristol License Agreement, we agreed to pay an initial amount of $37,500 upon the execution of the amended University of Bristol License Agreement, and additional amounts of up to $1.7 million, in the aggregate, tied to a financing milestone and to specific clinical development and commercialization milestones resulting from activities covered by the amended University of Bristol License Agreement, in addition to amounts under the original University of Bristol License Agreement of up to $3.2 million in the aggregate, tied to specific financing, development and commercialization milestones. Additionally, if we successfully commercialize any product candidate subject to the amended University of Bristol License Agreement or to the original University of Bristol License Agreement, we will be responsible, as provided in the original University of Bristol License Agreement, for royalty payments in the low-single digits and payments up to a percentage in the mid-teens of any sublicense income, subject to specified exceptions, based upon net sales of such licensed products. To date, we have paid the University of Bristol $50,000 pursuant to the University of Bristol License Agreement.
Unless otherwise terminated, the University of Bristol License Agreement will continue until the earlier of July 2036 or the expiration of the last patent claim subject to the University of Bristol License Agreement. We may terminate the University of Bristol License Agreement for convenience upon a specified number of days’ prior notice to the University of Bristol. The University of Bristol License Agreement will terminate under customary termination provisions including bankruptcy or insolvency or its material breach of the agreement. Under the terms of the University of Bristol License Agreement, we had provided 100 grams of cytisine to the University of Bristol as an initial contribution.
Ionis and UBC License Agreements
In August 2017, we discontinued further development of apatorsen. We provided a notice of discontinuance to our former development partners for apatorsen, Ionis Pharmaceuticals, Inc., or Ionis, and a letter of termination to the University of British Columbia, or UBC, notifying them that we have discontinued development of apatorsen resulting in termination of all licensing agreements related to this product candidate. We believe that all financial obligations, other than continuing mutual indemnification obligations and our requirement to pay for out-of-pocket patent expenses incurred up to the date of termination and for abandoning the apatorsen patents and patent applications, under all apatorsen related agreements with Ionis and UBC, are no longer owed and no further payments are due.
67
Assets and liabilities recorded at fair value in the balance sheets are categorized based upon the level of judgment associated with the inputs used to measure their fair value. For certain of our financial instruments including amounts receivable and accounts payable the carrying values approximate fair value due to their short-term nature.
ASC 820 “Fair Value Measurements and Disclosures,” specifies a hierarchy of valuation techniques based on whether the inputs to those valuation techniques are observable or unobservable. In accordance with ASC 820, these inputs are summarized in the three broad level listed below:
|
|
• |
Level 1 – Quoted prices in active markets for identical securities. |
|
|
• |
Level 2 – Other significant inputs that are observable through corroboration with market data (including quoted prices in active markets for similar securities). |
|
|
• |
Level 3 – Significant unobservable inputs that reflect management’s best estimate of what market participants would use in pricing the asset or liability. |
As quoted prices in active markets are not readily available for certain financial instruments, we obtain estimates for the fair value of financial instruments through third-party pricing service providers.
In determining the appropriate levels, we performed a detailed analysis of the assets and liabilities that are subject to ASC 820.
We invest our excess cash in accordance with investment guidelines that limit the credit exposure to any one financial institution other than securities issued by the U.S. Government. These securities are not collateralized and mature within one year.
A description of the valuation techniques applied to our financial instruments measured at fair value on a recurring basis follows.
Financial Instruments
Cash
Significant amounts of cash are held on deposit with large well established U.S. and Canadian financial institutions.
U.S. Government and Agency Securities
U.S. Government Securities U.S. government securities are valued using quoted market prices. Valuation adjustments are not applied. Accordingly, U.S. government securities are categorized in Level 1 of the fair value hierarchy.
U.S. Agency Securities U.S. agency securities are comprised of two main categories consisting of callable and non-callable agency issued debt securities. Non-callable agency issued debt securities are generally valued using quoted market prices. Callable agency issued debt securities are valued by benchmarking model-derived prices to quoted market prices and trade data for identical or comparable securities. Actively traded non-callable agency issued debt securities are categorized in Level 1 of the fair value hierarchy. Callable agency issued debt securities are categorized in Level 2 of the fair value hierarchy.
Corporate and Other Debt
Corporate Bonds and Commercial Paper The fair value of corporate bonds and commercial paper is estimated using recently executed transactions, market price quotations (where observable), bond spreads or credit default swap spreads adjusted for any basis difference between cash and derivative instruments. The spread data used are for the same maturity as the bond. If the spread data does not reference the issuer, then data that reference a comparable issuer are used. When observable price quotations are not available, fair value is determined based on cash flow models with yield curves, bond or single name credit default swap spreads and recovery rates based on collateral values as significant inputs. Corporate bonds and commercial paper are generally categorized in Level 2 of the fair value hierarchy; in instances where prices, spreads or any of the other aforementioned key inputs are unobservable, they are categorized in Level 3 of the hierarchy.
Warrants
As of December 31, 2017, we recorded a value of zero for our warrant liability. We reassess the fair value of the common stock warrants classified as liabilities at each reporting date utilizing a Black-Scholes pricing model. Inputs used in the pricing model include estimates of stock price volatility, expected warrant life and risk-free interest rate. The computation of expected volatility was
68
based on the historical volatility of comparable companies from a representative peer group selected based on industry and market capitalization. Warrants that are classified as liabilities are categorized in Level 3 of the fair value hierarchy. A small change in the estimates used may have a relatively large change in the estimated valuation. Warrants that are classified as equity are not considered liabilities and therefore are not reassessed for their fair values at each reporting date.
The following table presents the changes in fair value of our total Level 3 financial liabilities for the year ended December 31, 2017. During the twelve months ended December 31, 2017, no common stock warrants were issued that were classified as liabilities (in thousands):
|
|
|
Liability at |
|
|
Liability Assumed |
|
|
Unrealized |
|
|
Liability at |
|
||||
|
|
|
December 31, |
|
|
as part of |
|
|
Gain on |
|
|
December 31, |
|
||||
|
|
|
2016 |
|
|
Arrangement |
|
|
warrants |
|
|
2017 |
|
||||
|
Warrant liability |
|
$ |
— |
|
|
$ |
150 |
|
|
$ |
(150 |
) |
|
$ |
— |
|
The following table presents information about our assets and liabilities that are measured at fair value on a recurring basis, and indicates the fair value hierarchy of the valuation techniques we utilized to determine such fair value (in thousands):
|
December 31, 2017 |
|
Level 1 |
|
|
Level 2 |
|
|
Level 3 |
|
|
Total |
|
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
$ |
1,262 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
1,262 |
|
|
Money market securities (cash equivalents) |
|
|
4,022 |
|
|
|
— |
|
|
|
— |
|
|
|
4,022 |
|
|
Restricted cash (Note 12) |
|
|
272 |
|
|
|
— |
|
|
|
— |
|
|
|
272 |
|
|
Total assets |
|
$ |
5,556 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
5,556 |
|
|
Liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Warrants |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
December 31, 2016 |
|
Level 1 |
|
|
Level 2 |
|
|
Level 3 |
|
|
Total |
|
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
$ |
15 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
15 |
|
|
Total assets |
|
$ |
15 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
15 |
|
|
Liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Warrants |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
Cash and cash equivalents and short term investments (in thousands):
|
|
|
|
|
|
|
Gross |
|
|
Gross |
|
|
|
|
|
||
|
|
|
Amortized |
|
|
Unrealized |
|
|
Unrealized |
|
|
Estimated |
|
||||
|
December 31, 2017 |
|
Cost |
|
|
Gains |
|
|
Losses |
|
|
Fair Value |
|
||||
|
Cash |
|
$ |
1,262 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
1,262 |
|
|
Money market securities |
|
|
4,022 |
|
|
|
— |
|
|
|
— |
|
|
|
4,022 |
|
|
Total cash and cash equivalents |
|
$ |
5,284 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
5,284 |
|
|
Money market securities (restricted cash) |
|
|
272 |
|
|
|
— |
|
|
|
— |
|
|
|
272 |
|
|
Total restricted cash |
|
$ |
272 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
272 |
|
|
|
|
|
|
|
|
Gross |
|
|
Gross |
|
|
|
|
|
||
|
|
|
Amortized |
|
|
Unrealized |
|
|
Unrealized |
|
|
Estimated |
|
||||
|
December 31, 2016 |
|
Cost |
|
|
Gains |
|
|
Losses |
|
|
Fair Value |
|
||||
|
Cash |
|
$ |
15 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
15 |
|
|
Total cash and cash equivalents |
|
$ |
15 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
15 |
|
Our gross realized gains and losses on sales of available-for-sale securities were not material for the years ended December 31, 2017 and 2016.
All securities included in cash and cash equivalents have maturities of 90 days or less at the time of purchase. All securities included in short-term investments have maturities of within one year of the balance sheet date. The cost of securities sold is based on the specific identification method.
69
We only invest in A (or equivalent) rated securities with maturities of one year or less. We do not believe that there are any other than temporary impairments related to our investment in marketable securities at December 31, 2017, given the quality of the investment portfolio, its short-term nature, and subsequent proceeds collected on sale of securities that reached maturity.
9. PROPERTY AND EQUIPMENT
Property and equipment consisted of the following (in thousands):
|
|
|
|
|
|
|
Accumulated |
|
|
Net Book |
|
||
|
|
|
Cost |
|
|
Depreciation |
|
|
Value |
|
|||
|
December 31, 2017 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Computer equipment |
|
$ |
389 |
|
|
$ |
358 |
|
|
$ |
31 |
|
|
Furniture and fixtures |
|
|
157 |
|
|
|
156 |
|
|
|
1 |
|
|
Leasehold improvements |
|
|
252 |
|
|
|
226 |
|
|
|
26 |
|
|
Computer software |
|
|
322 |
|
|
|
321 |
|
|
|
1 |
|
|
Equipment under capital lease |
|
|
24 |
|
|
|
24 |
|
|
|
— |
|
|
Total property and equipment |
|
$ |
1,144 |
|
|
$ |
1,085 |
|
|
$ |
59 |
|
Impairment of Long-Lived Assets
We review long-lived assets for impairment whenever events or changes in circumstances indicate that the asset’s carrying amount may not be recoverable. We conduct our long-lived asset impairment analyses in accordance with ASC 360-10-15, “Impairment or Disposal of Long-Lived Assets.” ASC 360-10-15 requires us to group assets and liabilities at the lowest level for which identifiable cash flows are largely independent of the cash flows of other assets and liabilities and evaluate the asset group against the sum of the undiscounted future cash flows. If the undiscounted cash flows do not indicate the carrying amount of the asset is recoverable, an impairment charge is measured as the amount by which the carrying amount of the asset group exceeds its fair value based on discounted cash flow analysis or appraisals.
10. OTHER ASSETS
Other assets include deferred share issues costs, prepaid amounts related to insurance that will not be utilized in the next 12 months and deposits paid for office space in accordance with the terms of the operating lease agreements.
11. INCOME TAX
[a] On August 2, 2017, OncoGenex completed a reverse takeover with Achieve. OncoGenex changed its name to Achieve Life Sciences, Inc. We are a Delaware incorporated company subject to blended US Federal and state statutory rates for December 31, 2017, 2016 and 2015 of 34%, 34% and 34%, respectively. For the purposes of estimating the tax rate in effect at the time that deferred tax assets and liabilities are expected to reverse, management uses the furthest out available future tax rate in the applicable jurisdictions.
Income tax expense consisted of the following (in thousands):
70
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
||||
|
Income taxes at statutory rates (at a rate of 34% for all years presented) |
|
$ |
(4,636 |
) |
|
$ |
(504 |
) |
|
$ |
(407 |
) |
|
Expenses not deducted for tax purposes |
|
|
(174 |
) |
|
|
— |
|
|
|
— |
|
|
Effect of tax rate changes on deferred tax assets and liabilities |
|
|
3,158 |
|
|
|
— |
|
|
|
— |
|
|
Rate differential on foreign earnings |
|
|
314 |
|
|
|
— |
|
|
|
— |
|
|
Reduction in benefit of operating losses |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Reduction in the benefit of other tax attributes |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Investment tax credits |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Change in valuation allowance |
|
|
(1,683 |
) |
|
|
— |
|
|
|
— |
|
|
Book to tax return adjustments |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Other |
|
|
(14 |
) |
|
|
— |
|
|
|
— |
|
|
Income tax expense |
|
$ |
(3,035 |
) |
|
$ |
(504 |
) |
|
$ |
(407 |
) |
[b] At December 31, 2017, we have investment tax credits of $2.6 million (2016—$2.6 million) available to reduce future Canadian income taxes otherwise payable. We also have non-capital loss carryforwards of $120.4 million (2016—$115.9 million) available to offset future taxable income in Canada, UK net operating loss carryforwards of $0.8 million (2016—$0.2 million) to offset future taxable income in the UK and federal net operating loss carryforwards of $9.9 million (2016—$1.3 million) to offset future taxable income in the United States.
The investment tax credits and non-capital losses and net operating losses for income tax purposes expire as follows (in thousands):
|
|
|
|
|
|
|
US |
|
|
Canadian |
|
|
UK |
|
|||
|
|
|
Investment |
|
|
Net Operating |
|
|
Non-capital |
|
|
Net Operating |
|
||||
|
|
|
Tax Credits |
|
|
Losses |
|
|
Losses |
|
|
Losses |
|
||||
|
2022 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2023 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2024 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2025 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2026 |
|
|
244 |
|
|
|
— |
|
|
|
7,335 |
|
|
|
— |
|
|
2027 |
|
|
71 |
|
|
|
— |
|
|
|
4,949 |
|
|
|
— |
|
|
2028 |
|
|
148 |
|
|
|
— |
|
|
|
8,020 |
|
|
|
— |
|
|
2029 |
|
|
317 |
|
|
|
9 |
|
|
|
(9 |
) |
|
|
35 |
|
|
2030 |
|
|
346 |
|
|
|
5 |
|
|
|
6,288 |
|
|
|
21 |
|
|
2031 |
|
|
486 |
|
|
|
17 |
|
|
|
12,121 |
|
|
|
37 |
|
|
2032 |
|
|
363 |
|
|
|
43 |
|
|
|
17,278 |
|
|
|
43 |
|
|
2033 |
|
|
193 |
|
|
|
2 |
|
|
|
23,240 |
|
|
|
56 |
|
|
2034 |
|
|
215 |
|
|
|
3 |
|
|
|
17,077 |
|
|
|
48 |
|
|
2035 |
|
|
122 |
|
|
|
654 |
|
|
|
3,112 |
|
|
|
28 |
|
|
2036 |
|
|
79 |
|
|
|
611 |
|
|
|
16,664 |
|
|
|
3 |
|
|
2037 |
|
|
19 |
|
|
|
8,530 |
|
|
|
4,348 |
|
|
|
578 |
|
|
|
|
$ |
2,603 |
|
|
$ |
9,874 |
|
|
$ |
120,423 |
|
|
$ |
849 |
|
In addition, we have unclaimed tax deductions of approximately $15.5 million related to scientific research and experimental development expenditures available to carry forward indefinitely to reduce Canadian taxable income of future years. We also have research and development tax credits of $19,000 available to reduce future taxes payable in the United States. The research and development tax credits expire between 2018 and 2037.
71
[c] Significant components of our deferred tax assets as of December 31 are shown below (in thousands):
|
|
|
2017 |
|
|
2016 |
|
||
|
Deferred tax assets |
|
|
|
|
|
|
|
|
|
Tax basis in excess of book value of assets |
|
$ |
850 |
|
|
$ |
— |
|
|
Non-capital loss carryforwards |
|
|
33,524 |
|
|
|
496 |
|
|
Research and development deductions and credits |
|
|
5,506 |
|
|
|
— |
|
|
Stock options |
|
|
51 |
|
|
|
— |
|
|
§59(e) Capitalized R&D expenses |
|
|
3,252 |
|
|
|
— |
|
|
Accrued expenses |
|
|
— |
|
|
|
363 |
|
|
Other |
|
|
246 |
|
|
|
— |
|
|
Total deferred tax assets |
|
|
43,429 |
|
|
|
859 |
|
|
Valuation allowance |
|
|
(42,914 |
) |
|
|
(46 |
) |
|
Net deferred assets |
|
|
515 |
|
|
|
813 |
|
|
Deferred tax liabilities |
|
|
|
|
|
|
|
|
|
Intangible assets |
|
|
(513 |
) |
|
|
(937 |
) |
|
Other |
|
|
(2 |
) |
|
|
— |
|
|
Total deferred tax liabilities |
|
|
(515 |
) |
|
|
(937 |
) |
|
|
|
|
|
|
|
|
|
|
|
Net deferred tax assets |
|
|
— |
|
|
|
(124 |
) |
The potential income tax benefits relating to these deferred tax assets have not been recognized in the accounts as their realization did not meet the requirements of “more likely than not” under the liability method of tax allocation. Accordingly, a valuation allowance has been recorded and no deferred tax assets have been recognized in all jurisdictions as at December 31, 2017 and in the UK as of December 31, 2016.
[d] Under ASC 740, the benefit of an uncertain tax position that is more likely than not of being sustained upon audit by the relevant taxing authority must be recognized at the largest amount that is more likely than not to be sustained. No portion of the benefit of an uncertain tax position may be recognized if the position has less than a 50% likelihood of being sustained.
A reconciliation of the unrecognized tax benefits of uncertain tax positions for the year ended December 31, 2017 is as follows (in thousands):
|
|
|
Year ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
|||
|
Balance at January 1 |
|
$ |
715 |
|
|
$ |
699 |
|
|
$ |
683 |
|
|
Additions based on tax positions related to the current year |
|
|
— |
|
|
|
16 |
|
|
|
16 |
|
|
Additions based on tax positions related to prior years |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Balance at December 31 |
|
$ |
715 |
|
|
$ |
715 |
|
|
$ |
699 |
|
As of December 31, 2017, unrecognized benefits of approximately $0.7 million, if recognized, would affect our effective tax rate, and would reduce our deferred tax assets.
Our accounting policy is to treat interest and penalties relating to unrecognized tax benefits as a component of income taxes. As of December 31, 2017 and December 31, 2016 we had no accrued interest and penalties related to income taxes.
We are subject to taxes in Canada, the UK and the U.S. until the applicable statute of limitations expires. Tax audits by their very nature are often complex and can require several years to complete.
|
Tax |
|
Years open to |
|
Jurisdiction |
|
examination |
|
Canada |
|
2009 to 2017 |
|
United Kingdom |
|
2010 to 2017 |
|
US |
|
2009 to 2017 |
72
On December 22, 2017, the U.S. government enacted comprehensive tax legislation commonly referred to as the Tax Cuts and Jobs Act (the “Tax Act”). The Tax Act makes broad and complex changes to the U.S. tax code, including, but not limited to,
(1) reducing the U.S. federal corporate tax rate from 34 percent to 21 percent;
(2) eliminating the corporate alternative minimum tax;
(3) creating a new limitation on deductible interest expense; and
(4) changing rules related to uses and limitations of net operating loss carryforwards created in tax years beginning after December 31, 2017.
As a result of when the Act was signed into law, our deferred tax assets and liabilities were required to be remeasured using the lower 21% federal rate as of December 31, 2017.
12. COMMON STOCK
[a] Authorized
75,000,000 authorized common voting share, par value of $0.001, and 5,000,000 preferred shares, par value of $0.001.
[b] Issued and outstanding shares
Purchase Agreement and Financing with Lincoln Park Capital
On September 14, 2017 we and Lincoln Park Capital Fund, LLC, or LPC, entered into a share and unit purchase agreement, or Purchase Agreement, pursuant to which we have the right to sell to LPC up to $11.0 million in shares of our common stock, par value $0.001 per share, subject to certain limitations and conditions set forth in the Purchase Agreement.
Pursuant to the Purchase Agreement, LPC initially purchased 328,947 of our units, or the Units, at a purchase price of $3.04 per unit, with each Unit consisting of (a) one share of our Common Stock and (b) one warrant to purchase one-quarter of a share of Common Stock at an exercise price of $3.496 per share, or Warrant. Each Warrant is exercisable six months following the issuance date until the date that is five years and six months after the issuance date and is subject to customary adjustments. The Warrants were issued only as part of the Units in the initial purchase of $1.0 million and no warrants shall be issued in connection with any other purchases of common stock under the Purchase Agreement.
After the initial purchase, if our stock price is above $1.00, as often as every other business day over the 30-month term of the Purchase Agreement, and up to an aggregate amount of an additional $10.0 million (subject to certain limitations) of shares of common stock, we have the right, from time to time, in our sole discretion and subject to certain conditions to direct LPC to purchase up to 80,000 shares of common stock with such amounts increasing as the closing sale price of our common stock as reported on The NASDAQ Capital Market increases. The purchase price of shares of common stock pursuant to the Purchase Agreement will be based on prevailing market prices of common stock at the time of sales without any fixed discount, and we will control the timing and amount of any sales of common stock to LPC. In addition, we may direct LPC to purchase additional amounts as accelerated purchases if on the date of a regular purchase the closing sale price of the common stock is not below $2.00 per share. As consideration for entering into the Purchase Agreement, we issued to LPC 123,516 shares of common stock; no cash proceeds were received from the issuance of these shares.
From September 14, 2017 through December 31, 2017, we offered and sold 873,778 shares of our common stock pursuant to our Purchase Agreement with LPC, including the 328,947 shares that were part of the initial purchase of Units. These sales resulted in gross proceeds to us of approximately $2.0 million and offering expenses of $0.1 million. As of December 31, 2017 shares of our common stock having an aggregate value of approximately $9.0 million remained available for sale under this offering program.
Equity Award Issuances and Settlements
During the year ended December 31, 2017, we did not issue any shares of common stock to satisfy stock option exercises and issued 5,464 shares of common stock to satisfy restricted stock unit settlements, respectively, compared with the issuance of no shares of common to satisfy stock option exercises and restricted stock unit settlements, respectively, for the year ended December 31, 2016.
73
2017 Equity Incentive Plan
As of December 31, 2017, we had reserved, pursuant to the 2017 Equity Incentive Plan, or the 2017 Plan, 1,052,200 common shares for issuance upon exercise of stock options, currently outstanding, by employees, directors and officers of ours.
Under the 2017 Plan, we may grant options to purchase common shares or restricted stock units to our employees, directors, officers and consultants. The exercise price of the options is determined by our board of directors but will be at least equal to the fair value of the common shares at the grant date. The options vest in accordance with terms as determined by our board of directors, typically over three to four years for options issued to employees and consultants, and over one to three years for members of our board of directors. The expiry date for each option is set by our board of directors with a maximum expiry date of ten years from the date of grant. In addition, the 2017 Plan allows for accelerated vesting of outstanding equity awards in the event of a change in control. The terms for accelerated vesting, in the event of a change in control, is determined at our discretion and defined under the employment agreements for our officers and certain of our employees.
2010 Performance Incentive Plan
As at December 31, 2017 we had reserved, pursuant to our 2010 Performance Incentive Plan, 68,507 common shares for issuance upon exercise of stock options and settlement of restricted stock units by employees, directors, officers and consultants of ours, of which 63,447 are reserved for options currently outstanding and 5,060 are reserved for restricted stock units currently outstanding.
Under the 2010 Plan we granted options to purchase common shares and restricted stock units to our employees, directors, officers and consultants. The exercise price of the options was determined by our board of directors and was at least equal to the fair value of the common shares at the grant date. The options vest in accordance with terms as determined by our board of directors, typically over three to four years for options issued to employees and consultants, and over one to three years for members of our board of directors. The expiry date for each option is set by our board of directors with a maximum expiry date of ten years from the date of grant. In addition, the 2010 Plan allows for accelerated vesting of outstanding equity awards in the event of a change in control. The terms for accelerated vesting, in the event of a change in control, is determined at our discretion and defined under the employment agreements for our officers and certain of our employees
ASC 718 Compensation – Stock Compensation
We recognize expense related to the fair value of our stock-based compensation awards using the provisions of ASC 718. We use the Black-Scholes option pricing model as the most appropriate fair value method for our stock options and recognize compensation expense for stock options on a straight-line basis over the requisite service period. In valuing our stock options using the Black-Scholes option pricing model, we make assumptions about risk-free interest rates, dividend yields, volatility and weighted average expected lives, including estimated forfeiture rates of the options.
The expected life was calculated based on the simplified method as permitted by the SEC’s Staff Accounting Bulletin 110, Share-Based Payment. We consider the use of the simplified method appropriate because of the lack of sufficient historical exercise data following the reverse merger of OncoGenex. The computation of expected volatility was based on the historical volatility of comparable companies from a representative peer group selected based on industry and market capitalization. The risk-free interest rate is based on a U.S. Treasury instrument whose term is consistent with the expected life of the stock options. In addition to the assumptions above, as required under ASC 718, management made an estimate of expected forfeitures and is recognizing compensation costs only for those equity awards expected to vest. Forfeiture rates are estimated using historical actual forfeiture rates. These rates are adjusted on a quarterly basis and any change in compensation expense is recognized in the period of the change. We have never paid or declared cash dividends on our common stock and do not expect to pay cash dividends in the foreseeable future.
The estimated fair value of stock options granted in the respective periods was determined using the Black-Scholes option pricing model using the following weighted average assumptions:
|
|
|
2017 |
|
|
|
|
Risk-free interest rates |
|
|
1.95 |
% |
|
|
Expected dividend yield |
|
|
0 |
% |
|
|
Expected life |
|
6 years |
|
|
|
|
Expected volatility |
|
|
86.06 |
% |
|
74
The weighted average fair value of stock options granted during the year ended December 31, 2017 was $2.09.
The results for the periods set forth below included stock-based compensation expense in the following expense categories of the consolidated statements of loss (in thousands):
|
|
|
Year ended |
|||
|
|
|
December 31, |
|||
|
|
|
2017 |
|
|
|
|
Research and development |
|
$ |
107 |
|
|
|
General and administrative |
|
|
241 |
|
|
|
Total stock-based compensation |
|
$ |
348 |
|
|
Options vest in accordance with terms as determined by our board of directors, typically over three or four years for employee and consultant grants and over one or three years for board of director option grants. The expiry date for each option is set by our board of directors with, which is typically seven to ten years. The exercise price of the options is determined by our board of directors but is at least equal to the fair value of the share at the grant date.
Stock option transactions and the number of stock options outstanding are summarized below:
|
|
|
Number of |
|
|
Weighted |
|
||
|
|
|
Optioned |
|
|
Average |
|
||
|
|
|
Common |
|
|
Exercise |
|
||
|
|
|
Shares |
|
|
Price |
|
||
|
Balance, January 1, 2017 |
|
$ |
— |
|
|
$ |
— |
|
|
Additions from OncoGenex Plan |
|
|
113,451 |
|
|
|
96.38 |
|
|
Granted |
|
|
1,052,200 |
|
|
|
2.89 |
|
|
Expired |
|
|
(19,543 |
) |
|
|
114.53 |
|
|
Exercised |
|
|
— |
|
|
|
— |
|
|
Forfeited |
|
|
(30,461 |
) |
|
|
92.72 |
|
|
Balance, December 31, 2017 |
|
|
1,115,647 |
|
|
$ |
7.99 |
|
The following table summarizes information about stock options outstanding at December 31, 2017 regarding the number of ordinary shares issuable upon: (1) outstanding options and (2) vested options.
(1) Number of common shares issuable upon exercise of outstanding options:
|
|
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
Contractual |
|
||
|
|
|
|
|
|
|
Average |
|
|
Life |
|
||
|
Exercise Prices |
|
Number of Options |
|
|
Exercise Price |
|
|
(in years) |
|
|||
|
$2.89 - $6.95 |
|
|
1,052,200 |
|
|
$ |
2.89 |
|
|
|
9.58 |
|
|
$6.96 - $15.73 |
|
|
4,090 |
|
|
|
11.00 |
|
|
|
8.40 |
|
|
$15.74 - $20.63 |
|
|
17,983 |
|
|
|
20.46 |
|
|
|
7.38 |
|
|
$20.64 - $37.35 |
|
|
6,452 |
|
|
|
31.53 |
|
|
|
6.76 |
|
|
$37.36 - $128.64 |
|
|
2,451 |
|
|
|
84.08 |
|
|
|
5.75 |
|
|
$128.65 - $130.57 |
|
|
8,905 |
|
|
|
129.69 |
|
|
|
6.20 |
|
|
$130.58 - $134.81 |
|
|
6,450 |
|
|
|
131.45 |
|
|
|
5.19 |
|
|
$134.82 - $143.88 |
|
|
5,927 |
|
|
|
142.41 |
|
|
|
4.36 |
|
|
$143.89 - $185.85 |
|
|
7,019 |
|
|
|
172.70 |
|
|
|
3.01 |
|
|
$185.86 - $245.08 |
|
|
4,170 |
|
|
|
237.60 |
|
|
|
2.21 |
|
|
|
|
|
1,115,647 |
|
|
$ |
7.99 |
|
|
|
9.37 |
|
75
(2) Number common shares issuable upon exercise of vested options:
|
|
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
Contractual |
|
||
|
|
|
|
|
|
|
Average |
|
|
Life |
|
||
|
Exercise Prices |
|
Number of Options |
|
|
Exercise Price |
|
|
(in years) |
|
|||
|
$2.89 - $6.95 |
|
|
3,644 |
|
|
$ |
2.89 |
|
|
|
9.58 |
|
|
$6.96 - $15.73 |
|
|
4,090 |
|
|
|
11.00 |
|
|
|
8.40 |
|
|
$15.74 - $20.63 |
|
|
14,883 |
|
|
|
20.46 |
|
|
|
7.38 |
|
|
$20.64 - $37.35 |
|
|
5,432 |
|
|
|
31.25 |
|
|
|
6.77 |
|
|
$37.36 - $128.64 |
|
|
2,451 |
|
|
|
84.08 |
|
|
|
5.75 |
|
|
$128.65 - $130.57 |
|
|
8,758 |
|
|
|
129.69 |
|
|
|
6.20 |
|
|
$130.58 - $134.81 |
|
|
6,450 |
|
|
|
131.45 |
|
|
|
5.19 |
|
|
$134.82 - $143.88 |
|
|
5,927 |
|
|
|
142.41 |
|
|
|
4.36 |
|
|
$143.89 - $185.85 |
|
|
7,019 |
|
|
|
172.70 |
|
|
|
3.01 |
|
|
$185.86 - $245.08 |
|
|
4,170 |
|
|
|
237.60 |
|
|
|
2.21 |
|
|
|
|
|
62,824 |
|
|
$ |
91.79 |
|
|
|
5.95 |
|
As at December 31, 2017, the total unrecognized compensation expense related to stock options granted was $2.0 million, which is expected to be recognized into expense over a period of approximately 3.9 years.
The estimated grant date fair value of stock options vested during the years ended December 31, 2017, 2016 and 2015 was $0.6 million, zero and zero, respectively.
The aggregate intrinsic value of options exercised was calculated as the difference between the exercise price of the stock options and the fair value of the underlying common stock as of the date of exercise. The aggregate intrinsic value of options exercised for the years ended December 31, 2017, 2016 and 2015 was zero, zero and zero, respectively. At December 31, 2017, the aggregate intrinsic value of the outstanding options was zero and the aggregate intrinsic value of the exercisable options was zero.
[d] Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four year period. We also grant restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we are required to evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision. For the year ended December 31, 2017, $0.1 million of stock based compensation expense was recognized related to these awards.
The following table summarizes our restricted stock unit award activity during the year ended December 31, 2017:
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
Number |
|
|
Average |
|
||
|
|
|
of |
|
|
Grant Date |
|
||
|
|
|
Shares |
|
|
Fair Value |
|
||
|
Balance, January 1, 2017 |
|
|
- |
|
|
$ |
- |
|
|
Additions from OncoGenex Plans |
|
|
10,527 |
|
|
|
41.12 |
|
|
Granted |
|
|
205,100 |
|
|
|
2.89 |
|
|
Released |
|
|
(5,464 |
) |
|
|
44.25 |
|
|
Forfeited or expired |
|
|
(3 |
) |
|
|
25.37 |
|
|
Balance, December 31, 2017 |
|
|
210,160 |
|
|
$ |
3.73 |
|
As of December 31, 2017, we had approximately $0.6 million in total unrecognized compensation expense related to our restricted stock unit awards which is to be recognized over a weighted-average period of approximately 3.75 years.
76
The following is a summary of outstanding warrants to purchase common stock at December 31, 2017:
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
Outstanding |
|
|
Exercise |
|
|
|
||
|
|
|
and |
|
|
price per |
|
|
|
||
|
|
|
Exercisable |
|
|
Share |
|
|
Expiration Date |
||
|
(1) Series A Warrants issued in July 2014 financing |
|
|
252,721 |
|
|
|
44.000 |
|
|
July 2019 |
|
(2) Series B Warrants issued in July 2014 financing |
|
|
60,933 |
|
|
|
44.000 |
|
|
July 2019 |
|
(3) Series A-1 Warrants issued in April 2015 financing |
|
|
21,748 |
|
|
|
26.400 |
|
|
October 2020 |
|
(4) Warrants issued in September 2017 financing |
|
|
82,237 |
|
|
|
3.496 |
|
|
March 2023 |
No warrants were exercised for the year ended December 31, 2017. The Series A-1 Warrants assumed by us as part of the Arrangement and the warrants issued in the September 2017 financing are classified as equity. The Series A and Series B assumed by us as part of the Arrangement are classified as liabilities. The estimated fair value of warrants classified as liabilities is reassessed at each reporting date using the Black-Scholes pricing model.
|
|
|
As of |
|
|||||
|
|
|
December 31, |
|
|||||
|
Series A and Series B Warrant Valuation Assumptions |
|
2017 |
|
|
2016 |
|
||
|
Risk-free interest rates |
|
|
1.82 |
% |
|
|
— |
|
|
Expected dividend yield |
|
|
0 |
% |
|
|
— |
|
|
Expected life |
|
1.50 years |
|
|
|
— |
|
|
|
Expected volatility |
|
|
86 |
% |
|
|
— |
|
[f] 401(k) Plan
We maintain a 401(k) plan. Our securities are not offered as an investment option. Our shares are prohibited for inclusion our 401(k) plan, as well as any match of our shares to employee contributions.
[g] Loss per common share
The following table presents the computation of basic and diluted net loss attributable to common stockholders per share (in thousands, except per share and share amounts):
|
|
|
Years ended December 31, |
|
|||||||||
|
|
|
2017 |
|
|
2016 |
|
|
2015 |
|
|||
|
Numerator |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(10,583 |
) |
|
$ |
(1,234 |
) |
|
$ |
(828 |
) |
|
Denominator |
|
|
|
|
|
|
|
|
|
|
|
|
|
Weighted average number of common shares outstanding |
|
|
4,794,421 |
|
|
|
21,230 |
|
|
|
21,230 |
|
|
Basic and diluted net loss per common share |
|
$ |
(2.21 |
) |
|
$ |
(58.13 |
) |
|
$ |
(39.00 |
) |
As of December 31, 2017 a total of 1.7 million options, restricted stock units and warrants, respectively, have not been included in the calculation of potential common shares as their effect on diluted per share amounts would have been anti-dilutive.
13. RELATED PARTY TRANSACTIONS
We entered into a consulting agreement with Ricanto, Ltd., or Ricanto, on September 17, 2015 to provide strategic consulting and advice concerning clinical development, regulatory matters and business planning. Richard Stewart and Anthony Clarke together own 100% of Ricanto. Richard Stewart is our Chief Executive Officer, or CEO, Chairman of the Board, and a principal stockholder. Anthony Clarke is our Chief Scientific Officer, President, a board director, and a principal stockholder. We incurred consulting fees from Ricanto of $0.1 million during the nine months ended September 30, 2016. The consulting agreement with Ricanto was terminated on August 1, 2017, immediately prior to the closing of the Arrangement. We did not incur any consulting fees from Ricanto in 2017. As of December 31, 2016, we recorded amounts payable to Ricanto of $0.6 million in accrued liabilities on our
77
balance sheet. On July 18, 2017, Ricanto converted all amounts owed to it, totaling $0.6 million, into 475 shares of our common stock, prior to the closing of the Arrangement, par value $0.01. Pursuant to the terms of the Arrangement, each share was converted into, approximately, 359.3053 shares of OncoGenex’s common stock, or 170,670 shares of common stock post-conversion. As of December 31, 2017 we had no outstanding amounts payable to Ricanto.
During 2016 we borrowed $0.2 million in total principal amount through two notes payable dated April 20, 2016 and December 8, 2016 from Richard Stewart. The notes mature and are payable upon demand one year from the date of issuance. Interest accrues at an annual rate of 3.5%. As of December 31, 2016 the outstanding principal, included in shareholder loans with related parties, was $0.2 million and accrued interest payable was $3,000. On July 24, 2017, Richard Stewart converted the $0.2 million, representing the entire amounts of principal and accrued interest owed, into 146 shares of our common stock, prior to the closing of the Arrangement, par value $0.01. Pursuant to the terms of the Arrangement, each share was converted into, approximately, 359.3014 shares of OncoGenex’s common stock, or 52,458 shares of common stock post-conversion. As of December 31, 2017 we had no outstanding principal or accrued interest with the related party.
We borrowed $2.7 million on May 18, 2015, through a convertible promissory note payable to a Lender of ours. The note matures and is payable upon demand one year from the date of the note. Interest accrues at an annual rate of 3.5%. On September 30, 2015 the Lender converted $2.0 million in principal into 4,500 shares of our common stock, prior to the closing of the Arrangement, par value $0.01, and became a principal stockholder. On March 7, 2017 we borrowed $20,000 through a note payable to the Lender. The note matures and is payable upon demand one year from the date of issuance. Interest accrues at an annual rate of 3.5%. As of December 31, 2016, the outstanding principal balance, included in shareholder loans with related parties, was $0.7 million and had accrued interest payable of $35,000. On July 24, 2017, the Lender converted the remaining amounts in principal and accrued interest, totaling $0.8 million, into 586 shares of our common stock, prior to the closing of the Arrangement, par value $0.01. Pursuant to the terms of the Arrangement, each share was converted into, approximately, 359.3052 shares of OncoGenex’s common stock, or 1,827,426 shares of common stock post-conversion. As of December 31, 2017 we had no outstanding principal or accrued interest with the related party.
We entered into an employment agreement on May 11, 2015 with one of our principal stockholders to serve as our CEO. We terminated the employment agreement on December 31, 2016. From May 11, 2015 to December 31, 2016, we had not paid any salary specified in the employment agreement. Salary otherwise payable as at December 31, 2016 was $0.7 million and was accrued on our balance sheet as Accrued compensation. On July 19, 2017 we entered into a separation agreement with our former CEO. Pursuant to the separation agreement, for settlement of all salaries owed, we paid 238 shares of our common stock, prior to the closing of the Arrangement, representing 50% of the total amounts owed as accrued compensation and paid $0.4 million for the remaining 50%, subsequent to the closing of the Arrangement. Pursuant to the terms of the Arrangement, each share was converted into, approximately, 359.3025 shares of OncoGenex’s common stock, or 85,514 shares of common stock post-conversion. As of December 31, 2017 we had no outstanding principal or accrued interest with the related party.
We entered into an employment agreement on August 17, 2015 with one of our principal stockholders to serve as our Chief Financial Officer, or CFO. We terminated the employment agreement on December 31, 2016. From August 17, 2015 to December 31, 2016, we had not paid any salary specified in the employment agreement. Salary otherwise payable as at December 31, 2016 was $0.3 million and was accrued on our balance sheet as Accrued compensation. On July 20, 2017 we entered into a separation agreement with our former CFO. Pursuant to the separation agreement, for settlement of all salaries owed and as a separation payment, we paid 127 shares of our common stock, prior to the closing of the Arrangement, representing 50% of the total amounts owed as accrued compensation and paid $0.2 million for the remaining 50%, subsequent to the closing of the Arrangement . Pursuant to the terms of the Arrangement, each share was converted into, approximately, 359.2992 shares of OncoGenex’s common stock, or 45,631 shares of common stock post-conversion. As of December 31, 2017 we had no outstanding principal or accrued interest with the related party.
Michelle Griffin, the spouse of Scott Cormack, OncoGenex’s former CEO and a current member of our board of directors, entered into a consulting agreement in 2013 with OncoGenex, which was amended thereafter. Immediately prior to the closing of the Arrangement, the consulting agreement was terminated. Pursuant to the consulting agreement, OncoGenex was obligated to pay to the consultant a termination fee of $0.6 million, which was accrued in OncoGenex’s accrued liabilities immediately prior to the closing of the Arrangement. Subsequent to the closing of the Arrangement, we paid the full amount of the termination fees and no amounts were accrued on our balance sheet as at December 31, 2017.
78
14. COMMITMENTS AND CONTINGENCIES
The following table summarizes our contractual obligations as of December 31, 2017 (in thousands):
|
|
|
Total |
|
|
Less than 1 year |
|
|
1-3 years |
|
|
3-5 years |
|
|
More than 5 years |
|
|||||
|
Bothell office operating lease |
|
$ |
95 |
|
|
$ |
95 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Vancouver office operating lease |
|
$ |
71 |
|
|
$ |
71 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Seattle office operating lease |
|
$ |
433 |
|
|
$ |
117 |
|
|
$ |
291 |
|
|
$ |
25 |
|
|
$ |
— |
|
|
Leased equipment |
|
$ |
3 |
|
|
$ |
3 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Total |
|
$ |
602 |
|
|
$ |
286 |
|
|
$ |
291 |
|
|
$ |
25 |
|
|
$ |
— |
|
Lease Arrangements
We have an operating lease agreement for office space being used in Vancouver, Canada, which expires in September 2018. Pursuant to the operating lease agreement, we have the option to terminate the lease early without penalty at any time after January 1, 2017 so long as we provide three months prior written notice to the landlord.
The future minimum annual lease payments under the Vancouver lease is $71,000 in 2018.
In February 2015, we entered into an office lease with Grosvenor International (Atlantic Freeholds) Limited, or Landlord, pursuant to which we leased approximately 11,526 square feet located at 19820 North Creek Parkway, Bothell, Washington, 98011, commencing on February 15, 2015. The initial term of this lease will expire on April 30, 2018, with an option to extend the term for one approximately three-year period. Our monthly base rent for the premises will start at approximately $18,000 commencing on May 1, 2015 and will increase on an annual basis up to approximately $20,000. We received a construction allowance, for leasehold improvements that we made, of approximately $0.1 million. We will be responsible for 17% of taxes levied upon the building during each calendar year of the term. We delivered to the Landlord a letter of credit in the amount of $0.2 million, in accordance with the terms if the lease, which the Landlord may draw upon for base rent or other damages in the event of our default under this lease. In August 2015 we exercised our expansion option for an additional 2,245 square feet of office space, which commenced on August 1, 2015. We did not exercise our renewal option under the lease agreement and the lease will expire on April 30, 2018.
The remaining future minimum annual lease payments under the Bothell lease are as follows (in thousands):
|
2018 |
|
|
95 |
|
|
Total |
|
$ |
95 |
|
Consolidated rent and operating expense relating to both the Vancouver, Canada and Bothell, Washington offices for years ended December 31, 2017, 2016 and 2015 was $0.6 million, $0.9 million and $2.8 million, respectively.
On December 11, 2017, we entered into a lease, or New Lease, with 520 Pike Street, Inc., or Pike, pursuant to which we will lease approximately 3,187 square feet located at Suite 2250 at 520 Pike Tower, Seattle, Washington, 98101, commencing on March 1, 2018, or such later date on which Pike delivers exclusive possession of the premises to us; and further provided, that if such delivery does not occur by May 1, 2018, we have the right to terminate the agreement upon provision of notice. The initial term of the New Lease will expire at the end of the month on the third anniversary of the New Lease.
Our monthly base rent for the premises will start at approximately $11,685 commencing on March 1, 2018 and will increase on an annual basis up to approximately $12,397. In addition, we will also be obligated to pay a security deposit to Pike in the amount of $37,192, subject to periodic reductions in the amount of $12,397 after each of the first and second anniversaries of the New Lease, which Pike may retain for base rent or other damages, in the event of our default under the New Lease.
We may not assign or sublet all or any portion of the premises without the consent of Pike, and Pike shall be entitled to 50% of any profit which we may receive above and beyond the rental price of the New Lease. Upon receipt of notice of our intent to assign or sublease any portion of the leased premises, Pike may terminate that portion of the premises within 30 days, and provided, that if such portion constitutes 50% or more of the total square footage of the premises, Pike may terminate the New Lease in its entirety.
The future minimum annual lease payments under the New Lease are as follows (in thousands):
79
|
2018 |
|
|
117 |
|
|
2019 |
|
|
144 |
|
|
2020 |
|
|
148 |
|
|
2021 |
|
|
25 |
|
|
Total |
|
$ |
434 |
|
Guarantees and Indemnifications
We indemnify our officers, directors and certain consultants for certain events or occurrences, subject to certain limits, while the officer or director is or was serving at its request in such capacity. The term of the indemnification period is equal to the officer’s or director’s lifetime.
The maximum amount of potential future indemnification is unlimited; however, we have obtained director and officer insurance that limits our exposure and may enable us to recover a portion of any future amounts paid. We believe that the fair value of these indemnification obligations is minimal. Accordingly, we have not recognized any liabilities relating to these obligations as of December 31, 2017.
We have certain agreements with certain organizations with which it does business that contain indemnification provisions pursuant to which it typically agrees to indemnify the party against certain types of third-party claims. We accrue for known indemnification issues when a loss is probable and can be reasonably estimated. There were no accruals for or expenses related to indemnification issues for any period presented.
Material Changes in Financial Condition
|
|
|
December 31, |
|
|||||
|
(in thousands) |
|
2017 |
|
|
2016 |
|
||
|
Total Assets |
|
$ |
9,892 |
|
|
$ |
3,807 |
|
|
Total Liabilities |
|
|
2,013 |
|
|
|
3,197 |
|
|
Total Equity |
|
|
7,879 |
|
|
|
610 |
|
The increase in assets as at December 31, 2017 as compared to December 31, 2016 primarily relates to increase in cash and cash equivalents following the Arrangement. The decrease in liabilities as at December 31, 2017 compared to December 31, 2016 was primarily due to lower stockholder loans with related parties and lower accrued compensation
15. SEVERANCE CHARGES
As a requirement for the closing of the Arrangement, OncoGenex terminated the employment of one senior executive. Severance payable at the date of the transaction was $1.2 million and has been accounted for as part of the purchase price allocation (Note 4—Intangibles). The severance payable was settled following the completion of the Arrangement and no amounts were owing as at December 31, 2017.
80
16. QUARTERLY FINANCIAL INFORMATION (UNAUDITED)
The following table summarizes the unaudited statements of operations for each quarter of 2017 and 2016 (in thousands, except per share amounts):
|
|
|
March 31 |
|
|
June 30 |
|
|
September 30 |
|
|
December 31 |
|
||||
|
2017 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
61 |
|
|
|
62 |
|
|
|
825 |
|
|
|
2,153 |
|
|
General and administrative |
|
|
260 |
|
|
|
96 |
|
|
|
1,546 |
|
|
|
1,629 |
|
|
Total operating expenses |
|
|
321 |
|
|
|
158 |
|
|
|
2,371 |
|
|
|
3,782 |
|
|
Other income |
|
|
(8 |
) |
|
|
(11 |
) |
|
|
(7,025 |
) |
|
|
42 |
|
|
Recovery of deferred income taxes |
|
|
124 |
|
|
|
— |
|
|
|
2,927 |
|
|
|
— |
|
|
Net loss |
|
|
(205 |
) |
|
|
(169 |
) |
|
|
(6,469 |
) |
|
|
(3,740 |
) |
|
Basic and diluted net loss per share |
|
$ |
(9.66 |
) |
|
$ |
(7.96 |
) |
|
$ |
(0.90 |
) |
|
$ |
(0.32 |
) |
|
2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
65 |
|
|
|
72 |
|
|
|
69 |
|
|
|
80 |
|
|
General and administrative |
|
|
289 |
|
|
|
281 |
|
|
|
329 |
|
|
|
529 |
|
|
Total operating expenses |
|
|
354 |
|
|
|
353 |
|
|
|
398 |
|
|
|
609 |
|
|
Other income |
|
|
(6 |
) |
|
|
(7 |
) |
|
|
(7 |
) |
|
|
(4 |
) |
|
Recovery of deferred income taxes |
|
|
118 |
|
|
|
122 |
|
|
|
137 |
|
|
|
127 |
|
|
Net loss |
|
|
(242 |
) |
|
|
(238 |
) |
|
|
(268 |
) |
|
|
(486 |
) |
|
Basic and diluted net loss per share |
|
$ |
(11.40 |
) |
|
$ |
(11.21 |
) |
|
$ |
(12.62 |
) |
|
$ |
(22.89 |
) |
17. SUBSEQUENT EVENTS
From January 1, 2018 through March 1, 2018 we offered and sold 800,000 shares of our common stock pursuant to our Purchase Agreement with LPC. These sales resulted in gross proceeds to us of approximately $1.3 million. As of March 1, 2018 shares of our common stock having an aggregate value of approximately $7.6 million remained available for sale under this offering program
81
None.
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that material information required to be disclosed in our periodic reports filed or submitted under the Exchange Act, is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Our disclosure controls and procedures are also designed to ensure that information required to be disclosed in the reports we file or submit under the Exchange Act is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate, to allow timely decisions regarding required disclosure.
We carried out an evaluation, under the supervision and with the participation of our management, including the principal executive officer and the principal financial officer, of the effectiveness of the design and operation of the disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act. Based on that evaluation, our principal executive officer and principal financial officer concluded that our disclosure controls and procedures were effective as of the end of the period covered by this Annual Report on Form 10-K.
Changes in Internal Control Over Financial Reporting
We have not made any changes to our internal control over financial reporting (as defined in Rule 13a-15(f) and 15d-15(f) under the Exchange Act) during the quarter ended December 31, 2017 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over our financial reporting, as defined in Rule 13a-15(f) under the Exchange Act. Our internal control over financial reporting is a process designed under the supervision of our principal executive and principal financial officers to provide reasonable assurance regarding the reliability of financial reporting and the preparation of our financial statements for external reporting purposes in accordance with U.S. generally accepted accounting principles.
As of December 31, 2017, management assessed the effectiveness of our internal control over financial reporting based on the framework established in “Internal Control—Integrated Framework” issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) (2013 Framework). Based on this evaluation, management has determined that our internal control over financial reporting was effective as of December 31, 2017.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Not applicable.
82
The information required by this Item is set forth in our 2018 Proxy Statement to be filed with the SEC within 120 days of December 31, 2017, and is incorporated by reference into this Annual Report on Form 10-K by reference.
The information required by this Item is set forth in our 2018 Proxy Statement to be filed with the SEC within 120 days of December 31, 2017, and is incorporated by reference into this Annual Report on Form 10-K by reference.
The following table sets forth certain information regarding our equity compensation plans as of December 31, 2017:
|
|
|
(a) |
|
|
(b) |
|
|
(c) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
Number of securities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
remaining available for |
|
|
|
|
|
|
Number of securities to be |
|
|
|
|
|
|
future issuance under |
|
|
||
|
|
|
issued upon exercise of |
|
|
Weighted-average |
|
|
equity compensation |
|
|
|||
|
|
|
outstanding options, |
|
|
exercise price of |
|
|
plans (excluding |
|
|
|||
|
|
|
restricted stock units, |
|
|
outstanding options, |
|
|
securities reflected in |
|
|
|||
|
Plan category |
|
warrants and rights |
|
|
warrants and rights |
|
|
column (a)) |
|
|
|||
|
Equity compensation plans approved by security holders |
|
|
1,632,026 |
|
(1) |
$ |
7.28 |
|
(1) |
|
2,002,032 |
|
(1) |
|
Equity compensation plans not approved by security holders(2) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
Total |
|
|
1,632,026 |
|
|
$ |
7.28 |
|
|
|
2,002,032 |
|
|
|
(1) |
As of December 31, 2017, we maintained the following equity compensation plans, which were approved by security holders: (a) the 2000 Stock Incentive Plan, (b) the 2007 Performance Incentive Plan, (c) the 2010 Performance Incentive Plan and (d) 2017 Equity Incentive Plan. |
The information required by this Item is set forth in our 2018 Proxy Statement to be filed with the SEC within 120 days of December 31, 2017, and is incorporated by reference into this Annual Report on Form 10-K by reference.
The information required by this Item is set forth in our 2018 Proxy Statement to be filed with the SEC within 120 days of December 31, 2017, and is incorporated by reference into this Annual Report on Form 10-K by reference.
83
(1) Financial Statements
(2) All schedules are omitted because they are not required or the required information is included in the consolidated financial statements or notes thereto.
(3) Exhibits
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
|||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.1 |
|
|
8-K |
|
033-80623 |
|
2.1 |
|
January 5, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.2 |
|
|
8-K |
|
033-80623 |
|
10.1 |
|
July 19, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.1 |
|
Second Amended and Restated Certificate of Incorporation filed on May 24, 2013 |
|
8-K |
|
033-80623 |
|
3.1 |
|
May 29, 2013 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.2 |
|
Certificate of Amendment to Amended and Restated Certificate of Incorporation filed on May 21, 2015 |
|
8-K |
|
033-80623 |
|
3.1 |
|
May 22, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.3 |
|
|
8-K |
|
033-80623 |
|
3.1 |
|
August 2, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.4 |
|
|
8-K |
|
033-80623 |
|
3.2 |
|
August 2, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.5 |
|
|
8-K |
|
033-80623 |
|
3.1 |
|
November 1, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.6 |
|
|
8-K |
|
033-80623 |
|
3.1 |
|
January 5, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.1 |
|
|
10-Q |
|
000-21243 |
|
4.1 |
|
November 10, 2008 |
|
|
||
|
4.2 |
|
|
8-K |
|
033-80623 |
|
4.1 |
|
June 27, 2014 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.3 |
|
|
8-K |
|
033-80623 |
|
4.1 |
|
April 30, 2015 |
|
|
||
84
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
|||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.4 |
|
|
8-K |
|
033-80623 |
|
4.2 |
|
June 27, 2014 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.5 |
|
|
8-K |
|
033-80623 |
|
4.3 |
|
June 27, 2014 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.6 |
|
|
8-K |
|
033-80623 |
|
4.1 |
|
September 14, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.1 |
|
Sonus Pharmaceuticals, Inc. 2007 Performance Incentive Plan (the “2007 Plan”)†† |
|
DEF 14A |
|
000-21243 |
|
Appendix A |
|
April 3, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.2 |
|
Form of Sonus Pharmaceuticals, Inc. Stock Option Agreement (pertaining to the 2007 Plan)†† |
|
10-Q |
|
000-21243 |
|
10.1 |
|
November 9, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.3 |
|
OncoGenex Technologies Inc. Amended and Restated Stock Option Plan†† |
|
F-1 |
|
333-139293 |
|
10.1 |
|
December 13, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.4 |
|
Form of OncoGenex Pharmaceuticals, Inc. 2010 Stock Option Agreement†† |
|
8-K |
|
033-80623 |
|
10.1 |
|
June 14, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.5 |
|
Form of OncoGenex Pharmaceuticals, Inc. 2010 Restricted Stock Unit Agreement†† |
|
10-Q |
|
033-80623 |
|
10.2 |
|
November 3, 2011 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.6 |
|
OncoGenex Pharmaceuticals, Inc. 2010 Performance Incentive Plan, as amended and restated†† |
|
DEF 14A |
|
033-80623 |
|
Appendix A |
|
April 16, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.7a |
|
|
DEF 14A |
|
033-80623 |
|
Appendix A |
|
September 21, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.7b |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.7c |
|
Form of Achieve Life Sciences Restricted Stock Unit Agreement†† |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.8 |
|
|
DEF 14A |
|
033-80623 |
|
Appendix B |
|
September 21, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.9 |
|
Form of Indemnification Agreement for Officers and Directors of the Company†† (p) |
|
S-1 |
|
33-96112 |
|
10.19 |
|
September 25, 1995 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.10 |
|
Form of Indemnification Agreement between OncoGenex Technologies Inc. and Cindy Jacobs†† |
|
F-1 |
|
333-139293 |
|
10.7 |
|
December 13, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.11 |
|
Employment Agreement between the Company and Cindy Jacobs dated as of November 3, 2009†† |
|
10-Q |
|
033-80623 |
|
10.27 |
|
November 5, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.12 |
|
Employment Agreement between OncoGenex Pharmaceuticals, Inc. and John Bencich†† |
|
10-Q |
|
033-80623 |
|
10.1 |
|
November 10, 2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.13 |
|
|
S-4/A |
|
333-216961 |
|
10.21 |
|
May 3, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
85
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
|||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Variation of Contract, by and between Sopharma AD and Extab Corporation, dated May 14, 2015* |
|
S-4/A |
|
333-216961 |
|
10.22 |
|
May 3, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.15 |
|
|
S-4/A |
|
333-216961 |
|
10.23 |
|
May 3, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.16 |
|
Variation of Contract, by and between Sopharma AD and Extab Corporation, dated May 14, 2015* |
|
S-4/A |
|
333-216961 |
|
10.24 |
|
May 3, 2017 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.17 |
|
|
S-4/A |
|
333-216961 |
|
10.25 |
|
May 3, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.18 |
|
|
S-4/A |
|
333-216961 |
|
10.27 |
|
May 3, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.19 |
|
|
8-K |
|
033-80623 |
|
10.1 |
|
February 12, 2015 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.20 |
|
Lease by and between 520 Pike Street, Inc. and Achieve Life Sciences, Inc., dated December 11, 2018 |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.21 |
|
|
8-K |
|
033-80623 |
|
10.1 |
|
September 14, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.22 |
|
|
10-Q |
|
033-80623 |
|
10.1 |
|
November 9, 2017 |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21.1 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23.1 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24.1 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.1 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.2 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.1 |
|
|
|
|
|
|
|
|
|
|
X |
||
86
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
|||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.2 |
|
|
|
|
|
|
|
|
|
|
X |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.INS |
|
XBRL Instance Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.SCH |
|
XBRL Taxonomy Extension Schema Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.LAB |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
† |
Schedules and similar attachments to the Merger Agreement have been omitted pursuant to Item 601(b)(2) of Regulation S-K. The Company will furnish supplementally a copy of any omitted schedule or similar attachment to the SEC upon request. |
|
†† |
Indicates management contract or compensatory plan or arrangement. |
|
* |
Confidential portions of this exhibit have been omitted and filed separately with the Commission pursuant to an application for Confidential Treatment under Rule 24b-2 promulgated under the Securities Exchange Act of 1934, as amended. |
|
** |
The certifications attached as Exhibits 32.1 and 32.2 accompany to this Annual Report on Form 10-K pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, and shall not be deemed filed for purposes of Section 18 of the Securities Exchange Act of 1934, as amended. |
87
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this Report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
|
|
|
ACHIEVE LIFE SCIENCES, INC. |
||
|
|
|
|
|
(Registrant) |
||
|
|
|
|
|
|||
|
Date: March 1, 2018 |
|
|
|
By: |
|
/s/ RICHARD STEWART |
|
|
|
|
|
|
|
Richard Stewart |
|
|
|
|
|
|
|
Chairman and Chief Executive Officer |
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Scott Cormack and John Bencich, jointly and severally, as such person’s attorneys-in-fact, each with the power of substitution, for such person in any and all capacities, to sign any amendments to this Annual Report on Form 10-K, and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact, or his substitute or substitutes, may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
By: /s/ RICHARD STEWART |
|
Chairman and Chief Executive Officer |
|
Date: March 1, 2018 |
|
Richard Stewart |
|
|
|
|
|
|
|
|
||
|
By: /s/ JOHN BENCICH |
|
Executive Vice President, Chief Financial Officer and Chief Operating Officer |
|
Date: March 1, 2018 |
|
John Bencich |
|
|
|
|
|
|
|
|
||
|
By: /s/ SCOTT CORMACK |
|
Director |
|
Date: March 1, 2018 |
|
Scott Cormack |
|
|
|
|
|
|
|
|
||
|
By: /s/ ANTHONY CLARKE |
|
Director |
|
Date: March 1, 2018 |
|
Anthony Clarke |
|
|
|
|
|
|
|
|
||
|
By: /s/ MARTIN MATTINGLY |
|
Director |
|
Date: March 1, 2018 |
|
Martin Mattingly |
|
|
|
|
|
|
|
|
||
|
By: /s/ H. STEWART PARKER |
|
Director |
|
Date: March 1, 2018 |
|
H. Stewart Parker |
|
|
|
|
|
|
|
|
||
|
By: /s/ JAY MOYES |
|
Director |
|
Date: March 1, 2018 |
|
Jay Moyes |
|
|
|
|
|
By: /s/ DONALD JOSEPH |
|
Director |
|
Date: March 1, 2018 |
|
Donald Joseph |
|
|
|
|
88