10-K: Annual report pursuant to Section 13 and 15(d)
Published on March 9, 2016
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
|
x |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2015
Or
|
¨ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number 033-80623
OncoGenex Pharmaceuticals, Inc.
(Exact name of the registrant as specified in its charter)
|
Delaware |
|
95-4343413 |
|
(State or other jurisdiction of incorporation or organization) |
|
(I.R.S. Employer Identification No.) |
19820 North Creek Parkway, Bothell, Washington 98011
(Address of principal executive offices, including zip code)
(425) 686-1500
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
Title of Each Class |
|
Name of Exchange on Which Registered |
|
Common Stock, par value $0.001 per share |
|
The NASDAQ Capital Market |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such report), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
|
¨ |
|
Accelerated filer |
|
¨ |
|
|
|
|
|
|||
|
Non-accelerated filer |
|
¨ |
|
Smaller reporting company |
|
x |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act.). Yes ¨ No x
As of June 30, 2015, the aggregate market value of the registrant’s Common Stock held by non-affiliates of the registrant was $48,992,133. As of March 9, 2016, 29,812,998 shares of the registrant’s Common Stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive Proxy Statement to be filed with the Securities and Exchange Commission not later than April 30, 2016, in connection with the solicitation of proxies for its 2016 Annual Meeting of Stockholders, are incorporated by reference into Items 10, 11, 12, 13 and 14 of Part III hereof.
OncoGenex Pharmaceuticals, Inc.
Table of Contents
|
|
|
|
|
|
|
ITEM 1. |
|
|
3 |
|
|
ITEM 1A. |
|
|
25 |
|
|
ITEM 1B. |
|
|
41 |
|
|
ITEM 2. |
|
|
41 |
|
|
ITEM 3. |
|
|
42 |
|
|
ITEM 4. |
|
|
42 |
|
|
|
|
|
||
|
|
|
|
|
|
|
ITEM 5. |
|
|
43 |
|
|
ITEM 6. |
|
|
44 |
|
|
ITEM 7. |
|
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
|
45 |
|
ITEM 7A. |
|
|
59 |
|
|
ITEM 8. |
|
|
61 |
|
|
ITEM 9. |
|
CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
|
90 |
|
ITEM 9A. |
|
|
90 |
|
|
ITEM 9B. |
|
|
90 |
|
|
|
|
|
||
|
|
|
|
|
|
|
ITEM 10. |
|
|
91 |
|
|
ITEM 11. |
|
|
91 |
|
|
ITEM 12. |
|
SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
|
91 |
|
ITEM 13. |
|
CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
|
91 |
|
ITEM 14. |
|
|
91 |
|
|
|
|
|
||
|
|
|
|
|
|
|
ITEM 15. |
|
|
92 |
|
2
References in this Form 10-K to “OncoGenex Pharmaceuticals,” “OncoGenex,” the “Company,” “we,” “us” or “our” refer to OncoGenex Pharmaceuticals, Inc. and its wholly owned subsidiaries. The information in this Annual Report on Form 10-K contains certain forward-looking statements, including statements related to clinical trials, regulatory approvals, markets for our products, new product development, capital requirements and trends in our business that involve risks and uncertainties. Our actual results may differ materially from the results discussed in the forward-looking statements. Factors that might cause such a difference include those discussed in “Business,” “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” as well as those discussed elsewhere in this Annual Report on Form 10-K.
OVERVIEW OF OUR BUSINESS
We are an emerging leader in next generation cancer therapeutics. Our mission is to accelerate transformative therapies to improve the lives of people living with cancer and other serious diseases. We have developed a pipeline of late-stage product candidates that are designed to block the production of specific proteins that promote treatment resistance in cancer. We believe our therapies have the potential to redefine treatment outcomes in a variety of cancers. We have three product candidates in our pipeline: custirsen, apatorsen and OGX-225, each of which has a distinct mechanism of action and represents a unique opportunity for cancer drug development. Of the product candidates in our pipeline, custirsen and apatorsen are clinical-stage assets being evaluated in two phase 3 studies and four phase 2 studies, respectively.
Product Candidates Overview and Recent Developments
Our product candidates—custirsen, apatorsen and OGX-225—focus on mechanisms of treatment resistance in cancer patients and are designed to block the production of specific proteins that we believe promote treatment resistance and survival of tumor cells and are over-produced in response to a variety of cancer treatments. Our aim in targeting these particular proteins is to disable the tumor cell’s adaptive defenses, thereby rendering the tumor cells more susceptible to attack with a variety of cancer therapies. We believe this approach will increase survival time and improve the quality of life for cancer patients.
Custirsen
Custirsen is currently being evaluated in two phase 3 trials; one in patients with prostate cancer and one in patients with non-small cell lung cancer, or NSCLC. Custirsen is designed to inhibit the production of clusterin, a protein we believe promotes survival of cancer cells when overexpressed in a variety of tumors. We and collaborating investigators have conducted one phase 3 clinical trial and five phase 2 clinical trials to evaluate the ability of custirsen to enhance the effects of therapy in prostate, non-small cell lung and breast cancers. Results have been presented for each of these trials. Refer to the discussion below under the headings “Our Product Candidates—Custirsen—Current Custirsen Development Activities” and “Our Product Candidates—Custirsen—Summary of Results of Custirsen Clinical Trials” for further details.
3
Ongoing Phase 3 Custirsen Trials:
|
Trial |
|
Cancer Indication |
|
Treatment Combination(1) |
|
Status |
|
|
|
|
|
|
|
|
|
|
|
Metastatic castrate resistant prostate cancer – survival endpoint |
|
Cabazitaxel with and |
|
· Final intent to treat analysis expected in the third quarter of 2016 (2) · Passed final interim futility analysis in December 2015 · Prospectively defined subpopulation did not meet criteria, as reported in December 2015
|
|
|
|
|
|
|
|
|
|
|
|
Advanced non-small cell lung cancer – survival endpoint |
|
Docetaxel with and without |
|
· Final survival analysis expected in the first half of 2017 (2) · Passed final interim futility analysis in July 2015 · Passed first interim futility analysis in August 2014 · Patient enrollment ongoing
|


|
(1) |
In all of our prostate cancer clinical trials and in clinical practice for prostate cancer, docetaxel and cabazitaxel are administered in combination with prednisone. |
|
(2) |
Depending on timing of enrollment and/or event-driven final analyses. |
Apatorsen
Apatorsen is our product candidate designed to inhibit production of heat shock protein 27, or Hsp27, a cell-survival protein expressed in many types of cancers including bladder, non-small cell lung, pancreatic, prostate and breast cancers. Hsp27 expression is stress-induced, including by many anti-cancer therapies. Overexpression of Hsp27 is thought to be an important factor leading to the development of treatment resistance and is associated with metastasis and negative clinical outcomes in patients with various tumor types.
Hsp27 can also function as an immunomodulatory protein by a number of mechanisms that include altering important membrane expressed proteins on monocytes and immature dendritic cells; this alteration results in tumor-associated immune cells that are not functional in identifying and killing cancer cells. The induction of anti-inflammatory cytokines by Hsp27 may also play a role in down-regulating lymphocyte activation leading to additional unresponsive immune cells.
We and collaborating investigators have conducted, or are in the process of conducting, two phase 1 and seven randomized phase 2 clinical trials that have been designed to evaluate the ability of apatorsen to enhance various treatments in patients with bladder, lung, pancreatic and prostate cancers. Final results have been presented for the first completed phase 1 trial evaluating various cancers. Final results have been presented for two trials (phase 1 and phase 2) in bladder cancer and initial results for one phase 2 trial in prostate cancer and one phase 2 trial in pancreatic cancer. Refer to the discussion below under the headings “Our Product Candidates—Apatorsen—Current Apatorsen Development Activities” and “Our Product Candidates—Apatorsen—Summary of Results of Apatorsen Clinical Trials” for further details.
In 2013, we initiated the ORCA (Ongoing Studies Evaluating Treatment Resistance in CAncer) program, which encompasses clinical studies designed to evaluate whether inhibition of Hsp27 can lead to improved prognosis and treatment outcomes for cancer patients. Our goal is to advance cancer treatment by conducting clinical trials for apatorsen across multiple cancer indications including bladder, lung, pancreatic and prostate cancers. We are conducting parallel clinical trials to evaluate apatorsen in several cancer indications and treatment combinations to accelerate the development of apatorsen. As part of this strategy, we are supporting specific investigator-sponsored trials to allow assessment of a broader range of clinical indications for future OncoGenex-sponsored trials and possible market approval. The ORCA trials, with exception of the Pacific™ trial, are designed to provide information that will be useful for designing future phase 3 trials and may be used as supportive studies for registration, if applicable. Due to small sample sizes, data from these trials are not likely to result in statistically significant differences in either progression free survival, or PFS, or survival.
4
Ongoing Apatorsen Trials - The ORCA Program:

|
Trial |
|
Cancer Indication |
|
Treatment Combination |
|
Status |
|
|
|
|
|
|
|
|
|
|
|
Metastatic bladder cancer |
|
Docetaxel with and without |
|
· Final results expected in the second half of 2016 · Patient enrollment completed in September 2015 |
|
|
|
|
|
|
|
|
|
|
|
Advanced non-squamous NSCLC |
|
Carboplatin and pemetrexed |
|
· Survival data expected in the second half of 2016 · Top-line results on PFS reported in January 2016
|
|
|
|
|
|
|
|
|
|
|
|
Advanced squamous NSCLC |
|
Gemcitabine and |
|
· Patient enrollment ongoing
|
|
|
|
|
|
|
|
|
|
|
|
Castrate resistant prostate cancer |
|
Zytiga (abiraterone acetate) |
|
· Patient enrollment completed in March 2016.
|




In addition to the Borealis-1 and Borealis-2 clinical trials in metastatic bladder cancer in the ORCA program, we are evaluating apatorsen for the potential treatment of non-muscle invasive bladder cancer, or NMIBC. We have completed a pre-Investigational New Drug meeting with FDA in preparation for a separate Investigational New Drug, or IND, application to evaluate apatorsen for intravesical administration in combination with Bacillus Calmette-Guerin, or BCG, treatment in patients with NMIBC. FDA had no objection to the study population or classification of subpopulations in the proposed study design and deemed the proposed definitions of primary and secondary endpoints acceptable. Refer to the discussion below under the headings “Our Product Candidates—Apatorsen—Current Apatorsen Development Activities” and “Our Product Candidates—Apatorsen—Summary of Planned Apatorsen Clinical Trials” for further details.
OGX-225
OGX-225 is our product candidate designed to inhibit the production of Insulin Growth Factor Binding Proteins -2 and -5, or IGFBP-2 and IGFBP-5, two proteins that when overexpressed affect the growth of cancer cells. Increased IGFBP-2 and IGFBP-5 production are observed in many human cancers, including prostate, breast, colorectal, non-small cell lung, glioblastoma, acute myeloid leukemia, acute lymphoblastic leukemia, neuroblastoma, and melanoma. The increased production of these proteins is linked to faster rates of cancer progression, treatment resistance, and shorter survival duration in humans.
Preclinical studies with human prostate and breast cancer cells have shown that reducing IGFBP-2 and IGFBP-5 production with OGX-225 sensitized these tumor types to hormone ablation therapy or chemotherapy and induced tumor cell death. We have completed IND enabling toxicology studies for OGX-225.
Financial Overview
In 2015, we recognized $18.2 million in collaboration revenue attributable to a collaboration agreement with Teva. We have devoted substantially all of our resources to the development of our product candidates.
We incurred a loss for the year ended December 31, 2015 of $16.8 million and had an accumulated deficit at December 31, 2015 of $176.8 million and $58.2 million of total assets. We expect to continue to incur additional losses in the future as we continue our research and development activities.
To date, we have funded our operations primarily through private and public placements of equity securities as well as upfront payments and custirsen expense reimbursements received from the collaboration agreement with Teva Pharmaceutical Industries Ltd., or Teva, which was terminated in April 2015. Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement
5
for certain continuing research and development activities related to custirsen, an amount equal to $27.0 million less approximately $3.8 million, which reduction represented a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and April 24, 2015. We are responsible for all custirsen-related expenses incurred from and after January 1, 2015.
Based on our current expectations, we believe that our cash, cash equivalents, and short-term investments will be sufficient to fund our currently planned operations into the third quarter of 2017. Depending on timing of enrollment or event-driven final analyses, the expected key milestones and activities are as follows:
|
|
• |
|
Custirsen |
|
|
• |
|
Announcing AFFINITY trial results, the phase 3 trial evaluating a survival benefit for custirsen in combination with cabazitaxel as second-line chemotherapy in approximately 630 patients with castrate-resistant prostate cancer. The final analysis for the intent-to-treat population is expected in the third quarter of 2016. |
|
|
• |
|
Announcing ENSPIRIT trial results, the phase 3 trial evaluating a survival benefit for custirsen in combination with docetaxel as second-line chemotherapy in approximately 700 patients with non-small cell lung cancer. The final survival analysis is expected in the first half of 2017. |
|
|
• |
|
Apatorsen |
|
|
• |
|
Announcing Borealis-2 trial results, an investigator-sponsored, randomized phase 2 trial evaluating apatorsen in combination with docetaxel treatment compared to docetaxel treatment alone in patients with advanced or metastatic bladder cancer. Final results are expected in the second half of 2016. |
|
|
• |
|
Announcing Spruce trial results for the overall survival endpoint, the investigator-sponsored, randomized, placebo-controlled phase 2 trial evaluating apatorsen treatment with carboplatin and pemetrexed chemotherapy in patients with previously untreated advanced non-squamous NSCLC. Results are expected in the second half of 2016. |
|
|
• |
|
Preparing an investigational new drug application for FDA submission regarding apatorsen via intravesical administration in combination with Bacillus Calmette-Guerin (BCG) treatment in patients with non-muscle invasive bladder cancer. |
OUR PRODUCT CANDIDATES
We have two clinical-stage product candidates, custirsen in phase 3 and apatorsen in phase 2, and one preclinical-stage product candidate, OGX-225.
Custirsen
Overview of Custirsen
Through our clinical trials, we are treating cancer patients with custirsen with the goal of reducing clusterin production. Clusterin is a protein that is over-produced in several types of cancer and in response to many cancer treatments, including hormone ablation therapy, chemotherapy and radiation therapy. Preclinical and other data suggest that clusterin promotes tumor cell survival. Increased clusterin production has been linked to faster rates of cancer progression, treatment resistance and shorter survival duration. Since increased clusterin production is observed in many human cancers, including prostate, non-small cell lung, breast, ovarian, bladder, renal, pancreatic, colon, anaplastic large cell lymphoma and melanoma, we believe that custirsen may have broad market potential to treat many cancer indications and disease stages.
A broad range of preclinical studies have shown that reducing clusterin production with custirsen: (i) facilitates tumor cell death by sensitizing human prostate, non-small cell lung, breast, ovarian, bladder, renal and melanoma tumor cells to various chemotherapies; and (ii) sensitizes prostate tumor cells to hormone ablation therapy and sensitizes prostate and non-small cell lung tumor cells to radiation therapy. Preclinical studies also indicate that reducing clusterin production with custirsen re-sensitizes docetaxel-resistant prostate tumor cells to docetaxel.
Our phase 1 clinical trials evaluated the safety of custirsen and established a recommended dose of custirsen in combination with docetaxel (assessed two different docetaxel schedules), a gemcitabine and a platinum chemotherapy regimen and hormone ablation therapy. Docetaxel, mitoxantrone, cabazitaxel, gemcitabine and platinums (cisplatin and carboplatin) are all examples of chemotherapy agents. Clinical data from our phase 1 trial in prostate cancer patients demonstrated that weekly intravenous administration of custirsen resulted in drug distribution to prostate cancer tissue and over 92% inhibition of its target, clusterin mRNA, in prostate tumor cells in these patients at the 640mg dose, which was the highest dose evaluated in this clinical trial. This dose was determined by the clinical investigators to be well tolerated and therefore was established as the recommended dose.
6
We have conducted five phase 2 clinical trials and one phase 3 trial to evaluate the ability of custirsen to enhance the effects of therapy in patients with prostate, non-small cell lung and breast cancer. Data from each of the trials demonstrates that adding custirsen to therapy shows potential benefits, including:
|
|
· |
longer survival duration for patients with worse poor prognostic factors when custirsen was added to first-line docetaxel compared to first-line docetaxel alone in patients with metastatic CRPC (randomized phase 3 trial); |
|
|
· |
longer survival duration when custirsen was added to first-line docetaxel compared to first-line docetaxel alone in patients with CRPC (randomized phase 2 trial); |
|
|
· |
longer survival duration when custirsen was added to either mitoxantrone or docetaxel as second-line chemotherapy compared to survival duration observed in two prior published trials of CRPC patients receiving second-line chemotherapy and comparable survival compared to results observed with cabazitaxel; |
|
|
· |
decreased on-treatment serum clusterin levels compared to baseline levels of the patient population; analysis of study data found that lower serum clusterin levels during treatment were predictive of survival; |
|
|
· |
increased frequency of pain palliation when compared to results with either mitoxantrone or cabazitaxel second-line chemotherapy in the phase 3 TROPIC trial, and increased frequency and duration of pain palliation when custirsen was added to either mitoxantrone or docetaxel as second-line chemotherapy when compared to the frequency and duration of pain palliation observed in the TAX 327 Study for first-line chemotherapy alone in patients with CRPC; and |
|
|
· |
longer survival duration when custirsen was added to gemcitabine and a platinum-containing chemotherapy compared to the survival duration reported in prior published results from randomized clinical trials in NSCLC patients receiving gemcitabine and a platinum-containing chemotherapy. |
Refer to the discussion below under the heading “Summary of Results of Custirsen Clinical Trials” for further details including safety summary.
The U.S. Adopted Name for the custirsen drug product is custirsen sodium, which is the generic name.
Current Custirsen Development Activities
The following clinical trials are currently ongoing:
|
|
· |
The AFFINITY Trial: The phase 3 clinical trial to evaluate a survival benefit for custirsen in combination with cabazitaxel treatment as second-line chemotherapy in patients with CRPC. AFFINITY was initiated in August 2012 and completed enrollment of approximately 630 patients in September 2014. In January 2015, an interim futility analysis was completed and per recommendation of an Independent Data Monitoring Committee, or IDMC, the trial continued as planned. |
Exploratory analyses from the phase 3 SYNERGY trial showed a significant survival benefit in men who received custirsen and who were at increased risk for poor outcomes. Men with an increased risk for poor outcomes are identified as having two or more of five common features: poor performance status, elevated prostate specific antigen, or PSA, elevated lactate dehydrogenase, or LDH, decreased hemoglobin, and the presence of liver metastasis.
Based on these findings, we sought advice from regulatory authorities to amend the AFFINITY trial to include these learnings and to adjust the statistical analysis plan accordingly. Both the FDA and European Medicines Agency, or EMA, were supportive of the proposed amendment to the AFFINITY protocol and statistical analysis plan. The following protocol amendment was submitted in all participating countries where the trial is being conducted:
|
|
o |
The inclusion of a co-primary survival objective for evaluating survival benefit in a subpopulation of men who were at increased risk for poor outcomes as well as for all men enrolled into the study, known as the intent-to-treat (ITT) population. |
|
|
o |
A revised statistical analysis plan including the hypothesized hazard ratio, or HR, for the subpopulation who were at an increased risk for poor outcomes specified to be 0.69 with the critical HR ≤ 0.778. The hypothesized HR for the ITT population, remains unchanged as 0.75 with the critical HR ≤ 0.820. |
|
|
o |
The revised statistical analysis plan included an interim analysis for the ITT population at the same time as the final analysis for the subpopulation. This interim analysis had both futility and early efficacy criteria defined for the ITT population. |
The co-primary survival analysis for the poor prognostic subpopulation and the interim analysis for the ITT population in the AFFINITY trial were completed in December 2015. The co-primary survival results for the subpopulation of men who had multiple poor prognostic risk factors revealed that the combination of custirsen and cabazitaxel did not meet the rigorous criteria required to demonstrate an improvement in overall survival (hypothesized hazard ratio < 0.69, one-sided
7
p value < 0.015). Based on the interim analysis for the ITT population, the IDMC recommended that the trial continue as planned. Both the IDMC and we remain blinded to all analyses and final results are expected in the third quarter of 2016, depending on timing of the event-driven final ITT analysis.
|
|
· |
The ENSPIRIT Trial: The phase 3 clinical trial to evaluate a survival benefit for custirsen in combination with docetaxel treatment as second-line chemotherapy in patients with NSCLC. This trial was initiated in September 2012. |
The first interim futility analysis was completed in August 2014. A protocol amendment was submitted and approved by all regulatory agencies in participating countries, to amend the statistical design and analysis plan of the ENSPIRIT trial including the following:
|
|
o |
A revised statistical analysis plan including the hypothesized HR, to be 0.75 with the critical HR of ≤ 0.84, reducing the required sample size from 1,100 to 700 patients. This change maintained 90% power while assessing for a more clinically relevant survival benefit when adding custirsen to second-line docetaxel. |
|
|
o |
A revision to the final interim futility analysis with more rigorous criteria in order to continue the trial due to lack of futility. This was successfully completed in July 2015, and the trial continued as planned. |
|
|
o |
The inclusion of an additional objective to analyze survival outcome based on NSCLC histology as part of the other non-primary analyses. |
We believe these amendments, specifically the revised statistical thresholds, are more appropriately aligned to the interests of both treating clinicians and their patients. Based on current ENSPIRIT enrollment projections and the changes outlined in the protocol amendment, we believe final survival results could be available in the first half of 2017, depending on completion of enrollment and timing of the event-driven final analysis.
Custirsen has received Fast Track designation from the U.S. Food and Drug Administration, or FDA, for second-line treatment of metastatic CRPC when combined with cabazitaxel and prednisone and for the second-line treatment of advanced NSCLC when combined with docetaxel in patients with disease progression following treatment with a first-line, platinum-based chemotherapy doublet regimen.
Summary of Results of Custirsen Clinical Trials
One phase 3 and five phase 2 clinical trials have been conducted to evaluate the ability of custirsen to enhance the effects of therapy in patients with prostate, non-small cell lung and breast cancer. The following is a summary of the completed clinical trials evaluating custirsen in combination with chemotherapy.
Summary of Final Results of the SYNERGY Phase 3 Clinical Trial in Patients with metastatic CRPC
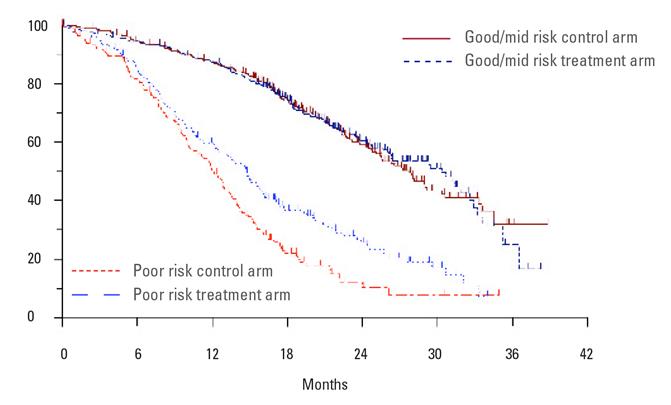
The trial enrolled 1,022 men at 124 sites across the United States and Europe between 2010 and 2012. Patients were randomized to receive either 640 mg of custirsen per week by intravenous infusion in combination with docetaxel or docetaxel alone, which remains the standard of care for first-line chemotherapy treatment in patients with metastatic CRPC. Top-line results were reported in April 2014 indicating that the addition of custirsen to first-line docetaxel chemotherapy did not meet the primary endpoint of a statistically significant improvement in overall survival in men with metastatic CRPC, compared to docetaxel alone (median survival 23.4 months vs 22.2 months, respectively; hazard ratio 0.93 and one-sided p value 0.207). However, subsequent exploratory analyses showed improved overall survival for men who had the worst poor prognostic scores and received custirsen. Prognostic scoring for each patient allowed classification into good, mid and poor prognostic subgroups. The figure below shows the survival difference for docetaxel plus custirsen treatment compared to docetaxel alone for the poor prognostic subgroup. For the good and mid prognostic subgroups combined, there was no survival difference for docetaxel plus custirsen treatment compared to docetaxel alone (also shown in the figure below).
In summary, exploratory analyses indicated a survival benefit in patients who had the worst prognostic scores based on a number of poor prognosis factors when treated with custirsen in combination with docetaxel compared to docetaxel alone:
|
|
· |
the exploratory multivariate analysis indicated that the significant predictors of overall survival in this study were low performance status, presence of liver metastases, opioid usage for prostate cancer pain, anemia, high levels of PSA in the blood as well as high blood levels of LDH and alkaline phosphatase, also known to be common poor prognostic laboratory indicators, and |
|
|
· |
the unadjusted hazard ratio, a measure used to compare the death rates between groups, showed a 27% lower rate of death for patients who were at increased risk for poor outcomes and received custirsen. |
8
As part of our phase 1, 2 and 3 clinical trials, custirsen has been administered to more than 1,300 patients with multiple types of cancer. Some of the patients experienced a variety of adverse events, the majority of which are associated with other treatments in the protocol and with the disease. The majority of adverse events were mild and the most common adverse events associated with custirsen consisted of flu-like symptoms. The most common moderate and severe adverse events occurring in more than 3% of patients who received custirsen and docetaxel in the completed phase 3 SYNERGY trial were fatigue, fever and neutropenia, weakness, diarrhea, pulmonary embolism (a blood clot that blocks an artery in the lungs), and pneumonia. These events also occurred in patients who received docetaxel alone in the completed phase 3 SYNERGY trial.
Summary of Final Results of Phase 2 Clinical Trial in Patients with CRPC Receiving Custirsen and Docetaxel as First-Line Chemotherapy
Final results of a randomized phase 2 trial evaluating the benefit of combining custirsen with first-line docetaxel in patients with CRPC were published in the September 20, 2010 issue of the Journal of Clinical Oncology, or JCO.
The trial enrolled 82 patients at 12 sites in Canada and the United States from September 2005 to December 2006. Patients were randomized to one of two treatment arms to receive either 640 mg of custirsen per week by intravenous infusion in combination with docetaxel or docetaxel alone. Analyses indicated a survival benefit in patients treated with custirsen in combination with docetaxel compared to docetaxel alone:
|
|
· |
median overall survival among patients treated with custirsen plus docetaxel was 23.8 months compared to 16.9 months for patients treated with docetaxel alone, indicating a 6.9 month survival advantage in the custirsen arm; |
|
|
· |
the unadjusted hazard ratio, a measure used to compare the death rates between treatment groups, was 0.61, representing a 39% lower rate of death for patients receiving custirsen; and |
|
|
· |
a prospectively defined multivariate analysis indicated that the significant predictors of overall survival in this study were treatment arm, performance status and presence of metastases other than in bone or lymph nodes. In the multivariate analysis, patients treated with custirsen had a rate of death 51% lower than patients treated with docetaxel alone (HR=0.49; p=0.012). |
9
Study investigators concluded that custirsen treatment was well tolerated in combination with docetaxel. Patients receiving custirsen had an increased incidence of mild fever, chills and elevated creatinine levels (a laboratory measure for reduced kidney function) and a moderate to significant decrease in circulating lymphocytes in the blood (another laboratory measure) without any increase in infection rate compared to patients receiving docetaxel alone. Lymphocytes are a type of white blood cell involved in the body’s defense against infections. Based on final results of this randomized phase 2 trial, the phase 3 SYNERGY trial was designed to evaluate the overall survival benefit of custirsen in patients treated with first-line chemotherapy.
Summary of Results of Phase 2 Clinical Trial in Patients Receiving Custirsen and Docetaxel as Second-Line Chemotherapy
Data from a phase 2 clinical study of custirsen in combination with docetaxel retreatment or mitoxantrone as second-line chemotherapy in patients with metastatic CRPC were published in the September 1, 2011 issue of Clinical Cancer Research, or CCR. In this phase 2 trial, patients who were previously treated with a first-line, docetaxel-based chemotherapy regimen and progressed on or within six months of discontinuation of docetaxel treatment were randomized to receive custirsen plus either docetaxel retreatment or mitoxantrone. Initially, 42 patients were randomized, received at least one cycle of custirsen and chemotherapy and were included in the analysis: 20 patients received docetaxel retreatment plus custirsen and 22 patients received mitoxantrone plus custirsen. The protocol was amended to allow additional patients to be enrolled in the docetaxel retreatment arm and 25 additional patients were enrolled.
Data from the clinical trial are summarized as follows:
|
|
· |
The median overall survival duration for the custirsen plus mitoxantrone arm was 11.5 months (95% C.I.: 6.1-15.2 months). For the custirsen plus docetaxel retreatment arm, the median overall survival was 15.8 months (95% C.I.:9.9-23.3 months) for the 20 randomized patients and 12.8 months (95% C.I.:9.9-17.0 months) for the combined patient population (n=45) that included 25 additional patients with high serum clusterin levels at enrollment beyond the 20 randomized patients. |
|
|
· |
Analyses presented in the CCR manuscript demonstrated that treatment with custirsen in combination with chemotherapy significantly lowered serum clusterin levels as compared to baseline levels, and that average serum clusterin levels during treatment were predictive of survival, with low serum clusterin levels correlating to longer survival. |
|
|
· |
Pain responses were observed in 62% of evaluable patients, with 88% of these patients having a durable response of three months or more. |
Summary of Results of Phase 2 Clinical Trial in Patients with NSCLC Receiving Custirsen and Gemcitabine/Platinum as First-Line Chemotherapy
Data from a phase 2 clinical study of custirsen in patients with advanced NSCLC was published in the January 2012 issue of Journal of Thoracic Oncology, or JTO. This study evaluated custirsen in combination with gemcitabine and a platinum chemotherapy (cisplatin or carboplatin) as first-line chemotherapy in 81 patients with advanced NSCLC. Eighty-one percent of the patients had stage IV disease at enrollment, and 16% had squamous cell carcinoma.
Data from the clinical trial are summarized as follows:
|
|
· |
the median overall survival was 14.1 months; |
|
|
· |
54% of patients survived at least one year; |
|
|
· |
30% of patients survived at least two years; |
|
|
· |
disease control was achieved in 69% of patients; and |
|
|
· |
analyses showed that treatment with custirsen in combination with gemcitabine and a platinum chemotherapy significantly lowered serum clusterin levels as compared to baseline levels, and that average serum clusterin levels during treatment were predictive of survival, with low serum clusterin levels correlating to longer survival. |
Summary of Preliminary Results of Phase 2 Clinical Trial in Patients with Advanced Breast Cancer Receiving Custirsen and Docetaxel as First- or Second-Line Chemotherapy
In January 2009, results of a phase 2 clinical trial in 15 patients with advanced breast cancer were published in the scientific journal CCR; this study evaluated custirsen in combination with docetaxel as first-line or second-line chemotherapy. The authors concluded that the combination of custirsen and docetaxel at 75 mg/m2 was well tolerated, and some clinical activity was seen in the patients with metastatic breast cancer.
10
Summary of Preliminary Results of Phase 2 Clinical Trial in Patients with CRPC Receiving Custirsen and Hormone Ablation Therapy
This trial was an investigator-sponsored trial that evaluated weekly custirsen with androgen withdrawal therapy for a three-month duration in patients with high-risk, localized prostate carcinoma prior to radical prostatectomy. Results of the trial indicated that custirsen was detectable in prostate tissue for 14 days after the last administration, that clusterin expression was decreased in cells from lymph nodes as well as from prostate specimens, and that patients who received custirsen plus androgen withdrawal therapy had higher levels of apoptosis (cell death) compared with patients who never received androgen withdrawal therapy or who received only androgen withdrawal therapy.
Summary of Results of Phase 3 Clinical Trial in Patients with CRPC Receiving a Taxane and Custirsen/Placebo Following Prior Docetaxel; Discontinued due to enrollment
Results of a randomized phase 3 trial evaluating the pain palliation benefit of custirsen in combination with taxane chemotherapy (docetaxel retreatment or cabazitaxel) in patients with CRPC following prior docetaxel were presented at the ASCO GU Symposium in January 2014. In this double-blind, placebo-controlled trial, called the SATURN trial, durable pain palliation for ³12 weeks duration was the primary endpoint.
The trial was stopped after 20 months, during which 14 subjects were randomized. Restrictive protocol-specified criteria of stable baseline pain and consistent analgesic use prevented the ability to complete trial enrollment.
Data from the clinical trial are summarized as follows:
|
|
· |
durable pain palliation of ³12 weeks duration was achieved in 3/14 subjects: n=1/7 (14%, taxane + placebo arm) and n=2/7 (29%, taxane + custirsen arm); |
|
|
· |
custirsen was generally well tolerated when administered in combination with a taxane (docetaxel or cabazitaxel) and prednisone; and |
|
|
· |
median (95% CI) overall survival by Kaplan-Meier analyses was 7.8 months (3.2, 11.5) (taxane + placebo) and 11.8 months (9.8, 15.7) (taxane + custirsen). |
Summary of Custirsen Development Program
Ongoing Phase 3 Custirsen Trials:
|
Cancer Indication and Trial |
|
Treatment Combination(1) |
|
Status |
|
Metastatic castrate resistant prostate cancer – survival endpoint (AFFINITY) |
|
Cabazitaxel with and without custirsen (~630 patients); second-line chemotherapy |
|
· Final intent to treat analysis expected in the third quarter of 2016 (2) · Passed final interim futility analysis in December 2015 · Prospectively defined subpopulation did not meet criteria, as reported in December 2015
|
|
|
|
|
|
|
|
Advanced non-small cell lung cancer – survival endpoint (ENSPIRIT) |
|
Docetaxel with and without custirsen (~700 patients); second-line chemotherapy |
|
· Final survival analysis expected in the first half of 2017 (2) · Passed final interim futility analysis in July 2015 · Passed first interim futility analysis in August 2014 · Patient enrollment ongoing |
11
Completed Custirsen Trials:
|
Cancer Indication |
|
Treatment Combination(1) |
|
Status |
|
Metastatic castrate resistant prostate cancer (SYNERGY) |
|
Docetaxel with and without |
|
· Completed; top-line data reported in April 2014; manuscript in preparation
|
|
|
|
|
|
|
|
Metastatic castrate resistant prostate cancer (SATURN) |
|
Taxane chemotherapy (docetaxel retreatment or cabazitaxel) with and without custirsen; second-line chemotherapy |
|
· Results presented at the ASCO GU Symposium in January 2014 · 14 patients enrolled in phase 3 · Phase 3 discontinued: Restrictive protocol-specified criteria of stable baseline pain and consistent analgesic use prevented the ability to complete trial enrollment. |
|
|
|
|
|
|
|
Metastatic castrate resistant prostate cancer |
|
Docetaxel with and without custirsen; first-line chemotherapy |
|
· Data published in JCO, September 2010 · Phase 2 completed |
|
|
|
|
|
|
|
Metastatic castrate resistant prostate cancer |
|
Docetaxel or mitoxantrone with and without custirsen; second-line chemotherapy |
|
· Data published in CCR, September 2011 · Phase 2 completed |
|
|
|
|
|
|
|
Advanced non-small cell lung cancer |
|
Gemcitabine and cisplatin or carboplatin with and without custirsen; first-line chemotherapy |
|
· Data published in JTO, January 2012 · Phase 2 completed |
|
|
|
|
|
|
|
Localized prostate cancer |
|
Custirsen with hormone ablation therapy |
|
· Results presented at ASCO 2008 Genitourinary Cancers Symposium · Phase 2 completed |
|
|
|
|
|
|
|
Advanced breast cancer |
|
Custirsen with docetaxel |
|
· Data published in CCR, January 2009 · Phase 2 completed |
|
|
|
|
|
|
|
Localized prostate cancer |
|
Custirsen with hormone ablation therapy |
|
· Data published in Journal of National Cancer Institute, September 2005 · Phase 1 completed |
|
|
|
|
|
|
|
Solid tumors (prostate, breast, NSCLC, ovarian, renal, bladder, peritoneum) |
|
Custirsen with docetaxel |
|
· Data published in CCR, February 2008 · Phase 1 completed |
|
(1) |
In all of our prostate cancer clinical trials and in clinical practice for prostate cancer, docetaxel and cabazitaxel are administered in combination with prednisone. |
|
(2) |
Depending on timing of enrollment and/or event-driven final analyses. |
Apatorsen
Overview of Apatorsen
Apatorsen is our product candidate that is designed to inhibit production of Hsp27, a cell-survival protein expressed in many types of cancers including bladder, prostate, breast, pancreatic and non-small cell lung cancer. Hsp27 expression is stress-induced, including by many anti-cancer therapies. Overexpression of Hsp27 is thought to be an important factor leading to the development of treatment resistance and is associated with metastasis and negative clinical outcomes in patients with various tumor types.
A number of preclinical studies have shown that reducing Hsp27 production induces tumor cell death in prostate, non-small cell lung, bladder and pancreatic cancer cells. The studies also suggest that reducing Hsp27 production sensitizes prostate tumor cells to hormone ablation therapy. These preclinical studies have also shown that inhibiting the production of Hsp27 in human prostate, bladder, lung, breast, ovarian and pancreatic tumor cells sensitizes the cells to chemotherapy.
Hsp27 has been reported by others to function as an immunomodulatory protein by a number of mechanisms that include altering important membrane expressed proteins on monocytes and immature dendritic cells; this alteration results in tumor-associated immune cells that are not functional in identifying and killing cancer cells. The induction of anti-inflammatory cytokines by Hsp27 may also play a role in down-regulating lymphocyte activation leading to additional unresponsive immune cells.
12
In 2013, we initiated the ORCA (Ongoing Studies Evaluating Treatment Resistance in CAncer) program which encompasses clinical studies designed to evaluate whether inhibition of Hsp27 can lead to improved prognosis and treatment outcomes for cancer patients. Our goal is to advance cancer treatment by conducting clinical trials for apatorsen across multiple cancer indications including bladder, lung, pancreatic and prostate cancers. We are conducting parallel clinical trials to evaluate apatorsen in several cancer indications and treatment combinations to accelerate the development of apatorsen. As part of this strategy, we are supporting specific investigator-sponsored trials to allow assessment of a broader range of clinical indications for future OncoGenex-sponsored trials and possible market approval. The ORCA trials, with exception of the Pacific™ trial, are designed to provide information that will be useful for designing future phase 3 trials and may be used as supportive studies for registration, if applicable. Due to small sample sizes, data from these trials are not likely to result in statistically significant differences in either PFS or survival.

Ongoing Trials
|
|
· |
The Borealis-2™ Trial: The investigator-sponsored, randomized phase 2 trial evaluating apatorsen in combination with docetaxel treatment compared to docetaxel treatment alone in patients with advanced or metastatic bladder cancer who have disease progression following first-line platinum-based chemotherapy. Patients may also continue weekly apatorsen infusions as maintenance treatment until disease progression or unacceptable toxicity if they complete all 10 cycles of docetaxel, or are discontinued from docetaxel due to docetaxel toxicity. This trial was initiated in April 2013 and patient enrollment was completed in September 2015. The trial randomized approximately 200 patients and results are expected in the second half of 2016. |
|
|
· |
The Spruce™ Trial: The investigator-sponsored, randomized, placebo-controlled phase 2 trial evaluating apatorsen plus carboplatin and pemetrexed therapy compared to carboplatin and pemetrexed therapy in patients with previously untreated advanced non-squamous NSCLC. Patients continued weekly apatorsen or placebo infusions as maintenance treatment until disease progression if they completed a minimum of 3 cycles of chemotherapy treatment. The aim of the trial is to determine if adding apatorsen to carboplatin and pemetrexed therapy can extend PFS outcome. Additional analyses are expected to include tumor response rates, overall survival, safety, tolerability and the effect of therapy on Hsp27 levels. Patients who are at increased risk for poor outcomes will also be prospectively evaluated. This trial was initiated in August 2013 and patient enrollment was completed in February 2015. The trial randomized approximately 155 patients. Primary endpoint data for PFS was reported in January 2016 and did not reach the statistical significance required to demonstrate a benefit. A potential PFS benefit was observed in patients with high baseline serum Hsp27 status when treated with apatorsen. The study is ongoing and overall survival results are expected in the second half of 2016. |
|
|
· |
The Spruce-2™ Trial (formerly referred to as the Cedar Trial): The investigator-sponsored, randomized phase 2 trial evaluating apatorsen plus gemcitabine and carboplatin therapy or gemcitabine and carboplatin therapy alone in patients with previously untreated advanced squamous NSCLC. Patients also continue weekly apatorsen infusions as maintenance treatment after chemotherapy until disease progression. The aim of the trial is to determine if adding apatorsen to gemcitabine and carboplatin therapy can extend PFS outcome. Additional analyses will include tumor response rates, overall survival, safety, and health-related quality of life. Additional analyses are expected to determine the effect of therapy on Hsp27 levels, explore potential biomarkers that may help predict response to treatment and survival outcomes in patients who were at increased risk for poor outcomes. The trial was initiated in July 2014 and is enrolling patients. The trial is expected to randomize approximately 140 patients. |
|
|
· |
The Pacific™ Trial: The investigator-sponsored, randomized phase 2 trial evaluating apatorsen in men with CRPC who are experiencing a rising PSA while receiving Zytiga® (abiraterone acetate). The aim of the trial is to determine if adding apatorsen to Zytiga treatment can reverse or delay treatment resistance by evaluating the PFS rate at a milestone Day 60 assessment. Other secondary endpoints such as PSA and objective responses, time to disease progression, CTCs and Hsp27 levels are expected to be evaluated. The trial completed enrollment of 72 patients in March 2016. |
13
Summary of Planned Apatorsen Clinical Trials
In addition to the Borealis-1 and Borealis-2 clinical trials in metastatic bladder cancer in the ORCA program, we are evaluating apatorsen for the potential treatment of NMIBC. We have completed a pre-IND meeting with FDA in preparation for a separate IND application to evaluate apatorsen for intravesical administration in combination with Bacillus Calmette-Guerin, or BCG, treatment in patients with NMIBC. FDA had no objection to the study population or classification of subpopulations in the proposed study design and deemed the proposed definitions of primary and secondary endpoints acceptable.
Summary of Completed Results of Apatorsen Clinical Trials
Preliminary or final results have been presented for a phase 1 clinical trial in patients with solid tumors, a phase 1 clinical trial in patients with superficial or muscle-invasive bladder cancer, a randomized phase 2 trial in metastatic CRPC, a randomized phase 2 in metastatic bladder cancer and a randomized phase 2 trial in metastatic pancreatic cancer. The following is a summary of the preliminary or final results from these trials.
Summary of Preliminary Results of Apatorsen Randomized Phase 2 Clinical Trial in Patients with Untreated Metastatic Pancreatic Cancer
Rainier enrolled and treated 130 patients with previously untreated metastatic pancreatic cancer. Patients were randomized to receive apatorsen in combination with ABRAXANE® (paclitaxel protein-bound particles for injectable suspension) (albumin-bound) and gemcitabine compared to ABRAXANE and gemcitabine alone. Patients were to receive up to six cycles of weekly intravenous therapy. The addition of apatorsen to ABRAXANE and gemcitabine did not demonstrate an overall survival benefit in the study when compared to ABRAXANE and gemcitabine alone. A potential benefit was observed in a subgroup of patients with high baseline serum Hsp27 status (14% of total) when treated with apatorsen (PFS HR= 0.40; 95% CI 0.19-0.86 and survival HR= 0.57; 95% CI 0.26-1.25). Overall, higher baseline Hsp27 status correlated with worse survival outcome. The study was sponsored and conducted by Sarah Cannon Research Institute, or SCRI, and further results were presented at the Gastrointestinal, or GI, Cancers Symposium meeting in January 2016. The study investigators concluded that these promising results in pancreatic cancer patients with high baseline Hsp27 status warrant further study of apatorsen in this population. We do not intend to pursue additional trials in pancreatic cancer at this time.
Summary of Preliminary Results of Apatorsen Randomized Phase 2 Clinical Trial in Patients with Metastatic Bladder Cancer
Borealis-1 enrolled and treated 179 patients with documented metastatic or locally inoperable transitional cell carcinoma, or TCC, of the urinary tract who had not previously received chemotherapy for metastatic disease and were not candidates for potentially curative surgery or radiotherapy. Patients were randomized to receive standard chemotherapy (gemcitabine/cisplatin) in combination with apatorsen at two dose levels (600 mg and 1000 mg) or gemcitabine/cisplatin plus placebo. Patients received up to six cycles of weekly intravenous therapy. Patients received weekly apatorsen or placebo maintenance therapy until disease progression or other reason for withdrawal from protocol treatment if they had completed a minimum of four cycles of chemotherapy. The primary endpoint of the trial was overall survival. Secondary endpoints included PFS, disease response and safety assessments for the two doses of apatorsen.
In December 2014, we announced overall trial results indicated that the addition of 600mg apatorsen to standard of care chemotherapy showed a 14% reduction in risk of death (overall survival hazard ratio (HR) = 0.86) and a 17% reduction in progressive disease and death (PFS HR = 0.83) when compared to chemotherapy alone. Subsequent exploratory analyses showed improved overall survival for those patients who received 600mg apatorsen and had poor prognosis over various prognostic factors such as performance status. Over one-third of the patients in the trial had lower performance status, as defined by a Karnofsky score of 80% or less. These patients derived the greatest benefit from 600mg apatorsen in combination with chemotherapy, resulting in a 50% reduction in risk of death (overall survival HR = 0.50) compared to chemotherapy alone. Less benefit was observed in the 1000mg apatorsen arm due to increased adverse events leading to a higher rate of discontinuation of both apatorsen and chemotherapy. Apatorsen 600mg was well tolerated in combination with chemotherapy. These data were presented at the 2015 ASCO Annual Meeting. We believe these results provide future direction for defining the patient population for a subsequent phase 3 trial.
Summary of Preliminary Results of Apatorsen Randomized Phase 2 Clinical Trial in Patients with CRPC
This randomized, controlled phase 2 trial completed enrollment of 74 patients who had minimally symptomatic or asymptomatic advanced prostate cancer and who have not yet received chemotherapy. The trial was designed to determine the potential benefit of apatorsen by assessing the number of patients without disease progression at 12 weeks post-study treatment with or without apatorsen. Preliminary study results presented at ESMO in September 2012 showed a higher number of patients without disease progression at 12 weeks and greater declines in PSA and CTCs in patients receiving apatorsen plus prednisone treatment compared to those receiving prednisone alone. A manuscript with final results is in development.
14
Apatorsen infusion reactions occurred and were primarily grade 1 or 2 chills, diarrhea, fatigue, nausea, flushing, pyrexia and vomiting. Other adverse events in two or more patients receiving apatorsen were dizziness, hot flashes, muscular weakness, and hypertension. Grade 3-4 laboratory treatment-emergent adverse events in two or more patients receiving apatorsen included lymphopenia (12%), hyperglycemia (12%), and elevated creatinine (6%).
Summary of Preliminary Results of Apatorsen Phase 1 Clinical Trial in Patients with Superficial Bladder Cancer
This investigator-sponsored phase 1 trial was designed to determine the effects of apatorsen on Hsp27 expression and tumor response rates when administered into the bladder using intravesical instillation. In addition, the trial measured the direct effect of delivering apatorsen by intravesical instillation on expression of Hsp27 in bladder tumor cells. This clinical trial was primarily funded by the National Cancer Institute of Canada.
Preliminary results from this trial were presented at the ASCO 2012 Genitourinary Cancers Symposium in February 2012 and demonstrated a trend towards decreased levels of Hsp27 and increased tumor cell death rates after intravesical treatment with apatorsen. In the apatorsen treated patients who experienced a complete pathologic response, the absence of residual disease made it difficult to fully assess the effect of apatorsen on Hsp27 expression. Therefore, the analysis was based mainly on the remaining patients who had evaluable tumor tissue. Results showed that eight of 24 patients (33%) had no pathologic evidence of disease. A manuscript with final results is in development.
Summary of Results of Apatorsen Phase 1 Clinical Trial in Patients with Solid Tumors
Apatorsen has been evaluated in a phase 1 trial in patients with breast, prostate, ovarian, or NSCLC who have failed potentially curative treatments or for whom a curative treatment does not exist. Final results of this phase 1 trial were presented in an oral presentation at the ASCO 2010 annual meeting. The phase 1 trial evaluated 42 patients treated with apatorsen as a single agent and 22 patients treated with apatorsen in combination with docetaxel who had failed up to six prior chemotherapy treatments. Apatorsen as a single agent administered weekly was evaluated at doses from 200 mg up to 1000 mg in five cohorts of approximately six patients per cohort. Two further cohorts evaluated apatorsen at the 800 and 1000 mg doses combined with docetaxel. Patients could receive up to 10 21-day cycles.
Most adverse events were mild (grade 1 or 2) and mainly occurred during the three “loading doses” given over nine days prior to weekly dosing. The most frequently reported adverse events in the apatorsen monotherapy arms were infusion-related reactions and chills. The most frequently reported adverse events in the apatorsen plus docetaxel arms were infusion-related reactions, chills, fatigue, diarrhea, pruritus (itching), nausea and back pain. The incidence of laboratory toxicity was determined based on laboratory data. The majority of laboratory toxicities were Grade 1 or Grade 2. Serious adverse events were reported for approximately half the patients. The most common events were disease progression and dyspnea (shortness of breath), reported for five subjects each, and febrile neutropenia, reported for four subjects. Increased blood creatinine (a test of kidney function) and hydronephrosis (obstruction of the urine flow from the kidney due to tumor blockage) were reported for two subjects each. All remaining serious adverse events were reported for one subject each.
Thirty patients had baseline and at least one post-baseline assessment of measurable disease. A total of eight of 30 patients (27%) had a decrease in measurable disease from baseline of at least 15%. For patients treated with monotherapy, three patients had tumor reductions and for patients treated with combined therapy with docetaxel, five patients had tumor reductions.
Thirty-three of 36 patients with prostate cancer had at least one post-baseline PSA. Three of 21 in the monotherapy cohorts had reductions in PSA greater than or equal to 30% as did six of 12 in the combination therapy cohorts. Six of seven patients with ovarian cancer had both baseline and post-baseline CA-125 (an ovarian tumor marker) measurements. All were treated with monotherapy. Three patients had a reduction of CA-125.
Decreases in both total CTCs and Hsp27+CTCs were observed. Hsp27+CTCs were decreased in 71% of evaluable patients.
In approximately 35% of patients, serum Hsp27 protein levels were decreased by 30% or greater over a time period of at least six weeks.
15
Summary of Apatorsen Development Program
Ongoing Apatorsen Trials:
|
Cancer Indication and Trial |
|
Treatment Combination |
|
Status |
|
Metastatic bladder cancer (Borealis-2) |
|
Docetaxel with and without apatorsen (~ 200 patients); second-line chemotherapy |
|
· Final results expected in the second half of 2016 · Patient enrollment completed in September 2015 |
|
|
|
|
|
|
|
Advanced non-squamous NSCLC (Spruce) |
|
Carboplatin and pemetrexed with and without apatorsen (~155 patients) |
|
· Survival data expected in the second half of 2016 |
|
|
|
|
|
· Top-line data on PFS reported in January 2016 |
|
|
|
|
|
|
|
Advanced squamous NSCLC (Spruce-2) |
|
Gemcitabine and carboplatin with and without apatorsen (~ 140 patients) |
|
· Patient enrollment ongoing |
|
|
|
|
|
|
|
Castrate resistant prostate cancer (Pacific) |
|
Zytiga (abiraterone acetate) with and without apatorsen (~72 patients) |
|
· Patient enrollment completed in March 2016. |
Completed Apatorsen Trials:
|
Cancer Indication |
|
Treatment Combination |
|
Status |
|
Metastatic pancreatic cancer (Rainier) |
|
Abraxane and gemcitabine with and without apatorsen (~ 130 patients) |
|
· Final data presented at 2016 GI ASCO · Top-line data reported in September 2015 · Phase 2 completed |
|
|
|
|
|
|
|
Metastatic bladder cancer (Borealis-1) |
|
Gemcitabine and cisplatin with and without apatorsen (~ 180 patients); first-line chemotherapy |
|
· Final data presented at 2015 ASCO Annual Meeting · Top-line data reported in December 2014 · Phase 2 completed |
|
|
|
|
|
|
|
Solid tumors |
|
Apatorsen with and without chemotherapy |
|
· Final data presented at 2010 ASCO Annual Meeting, manuscript accepted for publication · Phase 1 completed |
|
|
|
|
|
|
|
Superficial and muscle invasive bladder Cancer (BL-01) |
|
Apatorsen as monotherapy (24 patients) |
|
· Preliminary data presented at 2012 ASCO Genitourinary Cancers Symposium, manuscript in preparation · Phase 1 completed |
|
|
|
|
|
|
|
Castrate resistant prostate cancer (PR-01) |
|
Prednisone with and without apatorsen (74 patients) |
|
· Preliminary data presented at 2012 ESMO Annual Meeting, manuscript in preparation · Phase 2 completed |
OGX-225
Overview of OGX-225
OGX-225 is our product candidate designed to inhibit the production of Insulin Growth Factor Binding Proteins -2 and -5, or IGFBP-2, IGFBP-5, two proteins that when overexpressed affect the growth of cancer cells. Increased IGFBP-2 and IGFBP-5 production are observed in many human cancers, including prostate, breast, colorectal, non-small cell lung, glioblastoma, acute myeloid leukemia, acute lymphoblastic leukemia, neuroblastoma, and melanoma. The increased production of these proteins is linked to faster rates of cancer progression, treatment resistance, and shorter survival duration in humans.
16
Preclinical studies with human prostate and breast cancer cells have shown that reducing IGFBP-2 and IGFBP-5 production with OGX-225 sensitized these tumor types to hormone ablation therapy or chemotherapy and induced tumor cell death. We have completed IND enabling toxicology studies for OGX-225.
Summary of OGX-225 Development Program
OGX-225 Preclinical Studies:
|
Cancer Indication |
|
Treatment Combination |
|
Status |
|
Solid tumors |
|
OGX-225 with and without chemotherapy |
|
· Toxicology studies for initial IND completed · Preclinical proof-of-concept studies completed |
Second-Generation Antisense Technology
Custirsen, apatorsen and OGX-225 are based on second-generation antisense drug chemistry and belong to the drug class known as antisense therapeutics. On a product-by-product basis, we have collaborated with Ionis Pharmaceuticals, Inc. (formerly Isis Pharmaceuticals, Inc.), or Ionis, and selectively licensed technology from Ionis to combine Ionis’ second-generation antisense chemistry with our proprietary gene target sequences to create inhibitors that are designed to down-regulate certain proteins associated with cancer resistance. In contrast to first-generation antisense chemistry, second-generation antisense chemistry has improved target binding affinity, increased resistance to degradation, and improved tissue distribution. These improvements result in slower clearance of the therapies from the body, which allow for less frequent dosing and thereby make treatment easier on patients at a lower associated cost. For example, clinical data from our phase 1 clinical trial evaluating custirsen in combination with neoadjuvant hormone therapy in prostate cancer patients demonstrated that weekly intravenous administration of custirsen resulted in drug distribution to prostate cancer tissue and over 92% inhibition of its target, clusterin mRNA, in prostate tumor cells in these patients. These data demonstrate that, following systemic administration, custirsen entered tumor cells and effectively inhibited clusterin production.
OVERVIEW OF MARKET AND TREATMENT
In North America, cancer has recently surpassed heart disease as the leading cause of death in the United States. The American Cancer Society estimates that approximately 1.7 million new cancer cases are expected to be diagnosed in 2016. Cancer is the second most common cause of death in the United States, accounting for nearly 1 of every 4 deaths. Approximately 600,000 Americans are expected to die of cancer in 2016.
Typically, cancer treatments are given sequentially and can include hormone therapy, surgery, radiation therapy, immunotherapy and chemotherapy. Although a particular therapy may initially be effective, tumor cells often react to therapeutic treatment by increasing the production of proteins that afford them a survival advantage, enabling them to become resistant to therapy, multiply, and spread to additional organs. As a result, many patients progress through multiple different therapies and ultimately die from the disease.
OUR STRATEGY
Our objective is to develop and commercialize new cancer therapies that address resistance to therapies in cancer patients. Key elements of our strategy include:
|
|
· |
gaining market approval for custirsen by conducting registration trials that demonstrate efficacy and safety, in both prostate and lung cancer; |
|
|
· |
advancing apatorsen by conducting clinical trials across multiple cancer indications for apatorsen, including bladder, lung and prostate cancers. We are conducting parallel clinical trials to evaluate apatorsen in several cancer indications and treatment combinations to accelerate the development of apatorsen. We are supporting specific investigator-sponsored trials to allow assessment of a broader range of clinical indications for future OncoGenex-sponsored trials and possible market approval; |
17
|
|
· |
developing and commercializing new cancer therapies, including OGX-225, to inhibit treatment resistance in cancer patients. We plan to leverage our expertise in development to bring new products to market as soon as possible. We intend to maintain and develop our relationship with the Vancouver Prostate Centre and develop relationships with other research institutions in order to identify additional product candidates; and |
|
|
· |
optimizing the development of our product candidates through use of outsourcing and internal expertise. In order to increase efficiency and lower our overhead, we outsource, and plan to continue to outsource, preclinical and manufacturing activities. We have chosen to establish critical product development functions in-house, including clinical trial management and regulatory affairs. |
LICENSE AND COLLABORATION AGREEMENTS
Ionis Pharmaceuticals, Inc.
Custirsen
In November 2001, OncoGenex Technologies entered into an agreement with Ionis to jointly develop and commercialize custirsen. This strategic relationship provided us with access to Ionis’ proprietary position in second-generation antisense chemistry for use in custirsen, and Ionis’ expertise in developing antisense therapeutics, including its manufacturing expertise, and allowed us to develop custirsen cost efficiently. Under this agreement, we paid 65%, and Ionis paid 35%, of the costs resulting from the development and commercialization of custirsen. In July 2008, we and Ionis amended this agreement to provide that we are solely responsible for the costs and development of custirsen, and, in turn, we incurred certain financial obligations to Ionis, primarily related to sharing revenue received by us from a third party as a result of a licensing transaction.
Under the amended agreement, Ionis assigned to OncoGenex Technologies its rights in the patents claiming the composition and therapeutic methods of using custirsen, and granted OncoGenex Technologies a worldwide, nonexclusive license to their know-how and patents covering our core antisense technology and manufacturing technology solely for use with custirsen. The key product related patent that Ionis assigned to OncoGenex Technologies was U.S. Patent number 6,900,187 having an expiration date of at least 2021, and the key core antisense technology patents Ionis licensed OncoGenex Technologies are U.S. Patent number 7,919,472 having an expiration date of 2026 and its foreign equivalents pending in Australia, Canada, the European Patent Convention and Japan. In addition, Ionis agreed that so long as OncoGenex Technologies or its commercialization partner is using commercially reasonable efforts to develop and commercialize custirsen, Ionis will not research, develop or commercialize an antisense compound designed to modulate clusterin. The amended agreement will continue until OncoGenex Technologies or its commercialization partner is no longer developing or commercializing custirsen or until Ionis terminates the agreement for an uncured failure by OncoGenex Technologies to make a payment required under the agreement.
Licensing revenue that is based on a percentage of net sales of a licensor is defined as Royalty Revenue, while other licensing revenue, with the exception of fair market value of equity and reimbursement of research and development expenses, is defined as Non-Royalty Revenue. We will pay Ionis royalties comprised of a base percentage of net sales of custirsen and a percentage of Royalty Revenue we receive in excess of a certain threshold up to a certain cap. The amount of the royalties payable to Ionis depends on whether Ionis owes royalty payments to third parties pursuant to its license agreements with such parties. Our total royalty obligations to Ionis will depend on net sales of custirsen during the period and if Ionis owes royalty payments to third parties. In addition, we are required to pay Ionis 20% of all Non-Royalty Revenue we receive.
In May and November 2015, we received communications from Ionis requesting payment of 30% of the $23.2 million paid by Teva under the Termination Agreement, as well as 30% of any amounts paid by Teva upon release of the $3.0 million holdback amount. In January 2016, Ionis filed a lawsuit and claims that OncoGenex Technologies is in breach of the license agreement for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva in connection with the termination of the Collaboration Agreement. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the license agreement. We do not believe that any payments are due to Ionis. Under the Ionis license agreement, no payment is due to Ionis on any consideration that we receive for the reimbursement for research and development activities. The amounts paid or payable by Teva under the Termination Agreement constitute an advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, and therefore, no payments are owed to Ionis. We intend to vigorously defend the lawsuit and, based on our preliminary review, we believe we have valid defenses.
We paid Ionis $10 million in January 2010 as Ionis’ share of Non-Royalty Revenue received by us in December 2009 in connection with our collaboration agreement with Teva. We did not make any further payments to Ionis in 2015 under the terms of the agreement with Ionis.
18
Neither we nor Ionis can pursue the development or commercialization of any antisense compound for clusterin outside of the agreement with Ionis. This arrangement will continue until custirsen is no longer being developed or commercialized or until the agreement with Ionis is earlier terminated due to an uncured material breach.
To facilitate the execution and performance of the collaboration agreement with Teva, we and Ionis agreed to further amend our agreement, which amendment provided that, among other things, if we are the subject of a change of control with a third party, where the surviving entity immediately following such change of control has the right to develop and sell the product, then (i) a milestone payment of $20 million will be due and payable to Ionis 21 days following the first commercial sale of the product in the United States and (ii) unless such surviving entity had previously sublicensed the product and a royalty rate payable to Ionis by us has been established, the applicable royalty rate payable to Ionis will thereafter be the maximum amount payable under our agreement with Ionis. Any non-royalty milestone amounts previously paid will be credited towards the $20 million milestone if not already paid. As a result of the $10 million milestone payment paid to Ionis in relation to the collaboration agreement with Teva, the remaining amount owing in the event of change of control discussed above is a maximum of $10 million.
OncoGenex Technologies has agreed to indemnify Ionis and persons affiliated with Ionis against liabilities resulting from the development, manufacture, use, handling, storage, sale or other commercialization or disposition of custirsen caused by OncoGenex Technologies’ or its licensees’ or sublicensees’ gross negligence or willful misconduct, or caused by OncoGenex Technologies’ material breach of our agreement with Ionis.
Apatorsen
In January 2005, OncoGenex Technologies entered into a collaboration and license agreement with Ionis to jointly identify antisense compounds designed to inhibit the production of proteins encoded by specified gene targets. OncoGenex Technologies is solely responsible for all product development activities for antisense compounds under this collaboration. This relationship provides OncoGenex Technologies with access to Ionis’ proprietary position in second generation antisense chemistry for use in specified products. OncoGenex Technologies was permitted to designate up to two collaboration gene targets for collaborative research, development and commercialization. In April, 2005, Hsp27 was confirmed as a collaboration gene target, and we and Ionis jointly designed and screened antisense compounds for this gene target. OncoGenex Technologies’ right to designate a second collaboration gene target expired on January 5, 2007.
Under the terms of the agreement, in the event that OncoGenex Technologies abandons apatorsen, Ionis may elect to unilaterally continue development of apatorsen, in which case it must provide Ionis with a worldwide license or sublicense (as the case may be) of its relevant technology solely to develop and commercialize apatorsen in exchange for a royalty on Ionis’ sales of apatorsen.
Under the terms of the agreement, OncoGenex Technologies may be obligated to make certain milestone payments to Ionis contingent upon the occurrence of certain clinical development and regulatory events related to apatorsen. It is also obligated to pay to Ionis certain milestone payments, as well as certain low to mid-single digit royalties on net sales for apatorsen, with the amount of royalties depending on whether third-party royalty payments are owed. We paid Ionis USD$0.8 million in 2010 upon the initiation of a phase 2 clinical trial of apatorsen in patients with CRPC. We did not make any royalty payments to Ionis under the terms of the agreement in 2015.
OncoGenex Technologies has agreed to indemnify Ionis and certain persons affiliated with Ionis against liabilities caused by its and its licensees’ and sublicensees’ gross negligence or willful misconduct, its material breach of the collaboration and license agreement, and the manufacture, use, handling, storage, sale or other disposition of apatorsen that is sold by OncoGenex Technologies or its affiliates, agents or sublicensees.
The term of the collaboration and license agreement will continue for each product until the later of 10 years after the date of the first commercial sale of apatorsen and the expiration of the last to expire of any patents required to be licensed in order to use or sell apatorsen, unless OncoGenex Technologies abandons apatorsen and Ionis does not elect to unilaterally continue development of apatorsen.
University of British Columbia
Custirsen
Efforts conducted at the Vancouver Prostate Centre are owned and managed by the University of British Columbia, or UBC. Under a license agreement entered into in November 2001, as amended, UBC granted to OncoGenex Technologies an exclusive, worldwide license to commercialize its existing intellectual property and any improvements related to clusterin. This technology, combined with Ionis’ second-generation antisense chemistry, is our product candidate custirsen. In connection with entering into the license agreement, we issued to UBC shares of OncoGenex Technologies that were exchanged in the Arrangement for 15,243 shares of our common stock. OncoGenex Technologies agreed to pay UBC low single digit royalties on milestones and the revenue from sales of
19
custirsen. OncoGenex Technologies is obligated to pay UBC CAD$2,000 in annual maintenance fees. In January 2010, we paid UBC CAD$0.3 million as a result of upfront payments we received from Teva in December 2009 in connection with the collaboration agreement. The occurrence and receipt of future milestone payments and the generation of royalty revenue are uncertain. We did not make any royalty or milestone payments to UBC under the terms of the agreement in 2015.
OncoGenex Technologies agreed to use its commercially reasonable efforts to develop and exploit the licensed technology and any improvements. OncoGenex Technologies also agreed to promote, market and sell any resulting products and to cause the market demand for such products to be satisfied. OncoGenex Technologies is permitted to sublicense the technology, subject to certain consent and other requirements. OncoGenex Technologies directs patent prosecution and is responsible for all fees and costs related to the preparation, filing, prosecution and maintenance of the patent rights underlying the license agreement. OncoGenex Technologies indemnifies UBC and certain of UBC’s affiliates against liability arising out of the exercise of any rights granted pursuant to the agreement. The term of the agreement will expire on the later of 20 years from its effective date and the expiration of the last patent licensed under the agreement. Subject to patent term extensions, the current granted patent for custirsen expires in the United States in 2021 and would expire in all other jurisdictions by 2020. OncoGenex Technologies has additional patent applications pending that, if issued and not invalidated, may extend the expiration date of the last-to-expire patents. OncoGenex Technologies may also file additional patent applications related to clusterin that could potentially extend the expiration date of the last to expire patent in this area.
Apatorsen
Under a license agreement entered into in April 2005, as amended, UBC granted to OncoGenex Technologies an exclusive, worldwide license to commercialize its existing intellectual property and any improvements related to Hsp27. This technology, combined with Ionis’ second-generation antisense chemistry, is our product candidate apatorsen. In connection with entering into the license agreement, OncoGenex Technologies issued to UBC shares that were exchanged in the Arrangement for 6,533 shares of our common stock. OncoGenex Technologies also agreed to pay UBC low single digit royalties on the revenue from sales of apatorsen, which royalty rate may be reduced in the event that OncoGenex Technologies must pay additional royalties under patent licenses entered into with third parties in order to manufacture, use or sell apatorsen. OncoGenex Technologies may be obligated to make milestone payments to UBC contingent upon the occurrence of certain clinical development and regulatory events related to apatorsen. OncoGenex Technologies is obligated to pay UBC CAD$2,000 in annual maintenance fees. We paid UBC CAD$0.1 million in 2010 in relation to the initiation of a phase 2 trial of apatorsen in patients with CRPC. The occurrence and receipt of upfront and milestone payments and the generation of royalty revenue are uncertain. We did not make any royalty payments to UBC under the terms of the agreement in 2015.
Subject to certain exceptions, OncoGenex Technologies agreed to use its commercially reasonable efforts to (i) develop and exploit the licensed technology and any improvements and (ii) promote, market and sell any resulting products. OncoGenex Technologies is permitted to sublicense the technology, subject to certain consent and other requirements. OncoGenex Technologies directs patent prosecution and is responsible for all fees and costs related to the preparation, filing, prosecution and maintenance of the patent rights underlying the license agreement. OncoGenex Technologies indemnifies UBC and certain of UBC’s affiliates against liability arising out of the exercise of any rights granted pursuant to the agreement. The term of the agreement will expire on the later of 20 years from its effective date and the expiration of the last patent licensed under the agreement. Depending on the outcome of the pending patent applications in the licensed patent family, and subject to any applicable patent term extensions, a patent issuing from this family would expire in all jurisdictions by 2023. OncoGenex Technologies may also file additional patent applications related to Hsp27 that could potentially extend the expiration date of the last to expire patent in this area.
OGX-225
Pursuant to the terms of our third-party license agreement relating to OGX-225, we will owe payments upon the completion of product development milestones, as well as low to mid-single digit royalties on product sales. We did not make any milestone or royalty payments to third parties under the terms of the agreement in 2015.
We are also obligated to pay annual license fees to third parties with respect to these product candidates. These amounts are disclosed in “Management’s Discussion and Analysis of Financial Condition and Results of Operations – Contractual Obligations,” which is incorporated herein by reference.
20
Summary of Milestone Obligations by Product Candidate
The following table sets forth the milestones that we may be required to pay to third parties under the license and collaboration agreements described above. As described above, we will also be required to pay certain revenue-based royalties with respect to each of our product candidates.
|
Milestone Obligations to Third Parties |
|
Amount Payable |
|
Custirsen |
|
Up to 21% of non-royalty revenue (4) |
|
Apatorsen |
|
Up to $4,792,000 (1)(2)(3) |
|
OGX-225 |
|
Up to $4,115,000 (2)(3) |
|
(1) |
Additional milestone payments may be required for product approvals outside the field of oncology. |
|
(2) |
Payable in connection with initiating certain clinical trials and obtaining certain market approvals. |
|
(3) |
Certain milestone payments are payable in Canadian dollars, which are translated based on the December 31, 2015 exchange rate of US$1.00 = CAD$1.3840 and rounded to the nearest $1,000. |
|
(4) |
Dependent on future licensing and/or collaboration agreements with third parties. |
GOVERNMENT REGULATIONS
Drug Approval Process
Regulation by government authorities in the United States and other countries is a significant factor in our ongoing research and development activities and in the production and marketing of our products. In order to undertake clinical trials and to produce and market products for human use, mandatory procedures and safety standards established by the FDA in the United States and by comparable agencies in other countries must be followed.
The standard process before a pharmaceutical agent may be marketed includes the following steps:
|
|
· |
preclinical studies, including laboratory evaluation and animal studies to test for initial safety and efficacy; |
|
|
· |
submission to national health authorities of an IND or Clinical Trials Application, or CTA, or equivalent dossier, which must be accepted by each national health authority before human clinical trials may commence in that country; |
|
|
· |
adequate and well-controlled clinical trials to establish the safety and efficacy of the drug in its intended population and use(s); |
|
|
· |
submission to appropriate national and/or regional regulatory health authorities of a New Drug Application, or NDA, or equivalent marketing authorization application, which application is not automatically accepted for review; and |
|
|
· |
approval by appropriate regulatory health authorities of the marketing authorization application prior to any commercial sale or shipment of the drug in each country or jurisdiction. |
As part of the regulatory health authority approval for each product, the drug-manufacturing establishment is subject to inspection by the FDA and must comply with current Good Manufacturing Practices, or cGMP, requirements applicable to the production of pharmaceutical drug products. The facilities, procedures and operations of manufacturers must be determined to be adequate by the FDA before product approval.
Preclinical studies include laboratory evaluation of the active drug substance and its formulation in animals to assess the potential safety and efficacy of the drug and its formulation. Prior to initiating the first clinical testing of a new drug product candidate, the results of the preclinical studies are submitted to regulatory health authorities as part of an IND or CTA, and must be accepted before the proposed clinical trial(s) can begin.
Clinical trials for cancer therapeutics involve the administration of the investigational drug to patients with a defined disease state, under the supervision of a qualified principal investigator.
Clinical trials are conducted in accordance with protocols that detail the parameters to be used to monitor safety and efficacy. Each protocol is submitted to regulatory health authorities as part of the IND or CTA in each country where clinical trials are to be conducted. Each clinical trial is approved and monitored by independent Institutional Review Boards, or IRB, or Ethics Committees who consider ethical factors, informed consent documents, the safety of human subjects and the possible liability of the institutions conducting a clinical trial. The IRB or Ethics Committee may require changes in the clinical trials protocol, which may delay initiation or completion of the trial.
21
Clinical trials typically are conducted in three sequential phases, although the phases may overlap. In phase 1, the initial introduction of the drug to humans, the drug is tested for safety and clinical pharmacology. Phase 2 trials involve more detailed evaluation of the safety and efficacy of the drug in patients with a defined disease. Phase 3 trials consist of large-scale evaluations of safety and efficacy of the investigational drug compared to accepted standard therapy in a defined disease.
The process of completing clinical testing and obtaining regulatory approval for a new product takes a number of years and requires the expenditure of substantial resources. The FDA, or another regulatory authority, may not grant approval on a timely basis, if at all. We may encounter difficulties in securing regulatory approval or unanticipated costs, which may delay or preclude the commercialization of our product candidates. For instance, regulatory authorities may conclude that the data submitted in a marketing authorization application, such as a NDA, are not adequate to support approval of a pharmaceutical agent and may require further clinical and preclinical testing, re-submission of the application, and further review. Even after initial approval has been obtained, an indication may be limited or conditioned on the provision of further studies to support an approved indication, and further studies will be required to gain approval for the use of a product for clinical indications other than those for which the product was approved initially. Also, regulatory authorities require post-marketing surveillance programs to monitor the drug product’s side effects.
Marketing of pharmaceutical products outside of the United States is subject to regulatory requirements that vary from country to country. In the European Union, the general trend has been towards coordination of common standards for clinical testing of new drug products. Centralized approval in the European Union is coordinated through the EMA.
The level of regulation outside the United States and the European Union varies widely. The time required to obtain regulatory approval from regulatory agencies in each country may be longer or shorter than that required for FDA or EMA approval. In addition, in certain markets, reimbursement is subject to governmentally mandated prices.
CONTRACT RESEARCH AGREEMENTS
Consistent with our strategy to outsource certain product development activities, we have established contract research agreements for, preclinical, clinical, manufacturing and some data management services. We choose which business or institution to use for these services based on their expertise, capacity and reputation and the cost of the service.
We also provide quantities of our product candidates to academic research institutions to investigate the mechanism of action and evaluate novel combinations of product candidates with other cancer therapies in various cancer indications. These collaborations expand our research activities for product candidates with modest contribution from us.
RESEARCH AND DEVELOPMENT EXPENDITURES
For the years ended December 31, 2015, 2014 and 2013, our expenditures for research and development activities were $25.1 million, $46.2 million and $55.3 million, respectively. Such research and development expenses primarily related to the advancement of our product candidates custirsen and apatorsen.
MANUFACTURING
We do not own facilities for the manufacture of materials for clinical or commercial use. We rely and expect to continue to rely on contract manufacturers to manufacture our product candidates in accordance with cGMP, for use in clinical trials, as well as for process development as required. We will ultimately depend on contract manufacturers for the manufacture of our products, when and if we have any, for commercial sale.
To date, all active pharmaceutical ingredient, or API, and drug product for custirsen and apatorsen has been manufactured by third parties on a purchase order basis, under cGMP. If our product candidates are approved for commercial sale in the future, we may be required to contract with larger contract manufacturers that can meet higher commercial drug quantities.
INTELLECTUAL PROPERTY
Our success depends in part on our ability and that of our collaborators to obtain and maintain proprietary protection for our product candidates, technology, and know-how, to prevent others from infringing on the proprietary rights of our product candidates, and to operate without infringing on the proprietary rights of others.
22
Patents
We have a license from UBC and Ionis to use, make, have made, or make improvements upon custirsen, apatorsen and OGX-225. In addition, Ionis has assigned a three-member patent family related to clusterin antisense to OncoGenex Technologies, and we have a pending family of applications on an apatorsen formulation.
We have been granted non-exclusive rights to all intellectual property owned, licensed or otherwise controlled by Ionis as of the date of our agreements with Ionis that relate to second-generation antisense chemistry and that are required for our product candidates (such as custirsen, apatorsen and OGX-225). Ionis is generally restricted from engaging in research, development and commercialization of antisense compounds related to clusterin, Hsp27, IGFBP-5 and IGFBP-2, other than as provided in the collaboration and license agreement related to each target. Ionis directs patent prosecution and is responsible for all fees and costs related to the preparation, filing, prosecution and maintenance of these patent rights, which extend to numerous jurisdictions throughout the world. Individual patents have terms of protection depending on the laws of the countries in which the applications are made.
We direct patent prosecution, and are responsible for all fees and costs related to the preparation, filing, prosecution and maintenance of the patent rights for intellectual property under license from UBC covering custirsen, apatorsen and OGX-225. We file patent applications for this intellectual property in the United States, Canada, Europe (through the European Patent Office), Japan and other jurisdictions.
Composition of matter patents covering custirsen, apatorsen and OGX-225 have been issued in the United States and certain other jurisdictions. Additional patent applications covering all of these products, as well as other technologies, are pending in the United States and certain other countries.
Generally, patents issued in the United States are effective for 20 years from the earliest non-provisional filing date, if the application from which the patent issues was filed on or after June 8, 1995 (otherwise the term is the longer of 17 years from the issue date and 20 years from the earliest non-provisional filing date). The duration of patent terms for non-U.S. patents is typically 20 years from the earliest corresponding national or international filing date. Our licensed UBC patent estate, based on those patents and applications existing now and expected by us to issue, will expire in years ranging from 2020 to 2024, which dates do not include extensions that may be available. Patent term extensions, specifically to make up for regulatory delays, are available in the United States, Europe and Japan. Although we believe that some or all of our product candidates will meet the criteria for patent term extensions, we can provide no assurance that we will obtain such extensions.
We also rely on unpatented trade secrets, proprietary know-how and continuing technological innovation, which we seek to protect, in part, by confidentiality agreements with our corporate partners, collaborators, employees and consultants in our drug development research. We can provide no assurance that these agreements will not be breached, that we will have adequate remedies for any breach, or that our trade secrets or know-how will not otherwise become known or be independently discovered by competitors. Further, we can provide no assurance that we will be able to protect our trade secrets or that others will not independently develop substantially equivalent proprietary information and techniques.
Trademarks
We own several trademarks registered in the United States, including word marks ONCOGENEX™, ORCA™, Spruce™, and Rainier™, and design marks ORCA, Pacific, Borealis-1, Borealis-2, and the helical totem element that accompanies the clinical trial trademarked identifiers. In Canada, we have corresponding trademark registrations for all but Rainier™, which is pending. As requested by Cedars-Sinai, we have cancelled our trademark for the Cedar design in the United States and Canada.
We can provide no assurance that our registered or unregistered trademarks or trade names will not infringe upon third-party rights or will be acceptable to regulatory agencies.
COMPETITION
The life sciences industry is highly competitive, and we face significant competition from many pharmaceutical, biopharmaceutical and biotechnology companies that are researching and marketing products designed to address cancer indications for which we are currently developing products or for which we may develop products in the future. We are aware of several other companies which are developing therapeutics that seek to promote tumor cell death. Several therapies have been recently approved by the FDA, and we expect more to be approved in the future.
Many oncology drugs in clinical trials are being developed for the four primary indications: lung, breast, colorectal, and prostate cancers. Certain of these drugs are designed, like custirsen, apatorsen and OGX-225, to interfere with mechanisms potentially involved with treatment resistance. If new drugs targeting mechanisms of treatment resistance are approved for sale for the indications
23
that we are evaluating in advance of our product candidates or even after their commercialization, the market’s interest in our product candidates may be reduced. We are aware of several other companies developing therapeutic products, whether antisense or otherwise, which seek to promote tumor cell death by inhibiting proteins believed to promote cell survival. Our competitors may seek to identify gene sequences, protein targets or antisense chemistry different from ours, and outside the scope of our intellectual property protection, to develop antisense therapeutics that serve the same function as our product candidates. Our competitors may also seek to use mechanisms other than antisense to inhibit the proteins that our product candidates are designed to inhibit.
Some of our product candidates’ development plans include pursuing prostate and lung cancer indications. Substantial advancements in the treatment of prostate and lung cancer have occurred in the past two years and new products from our competitors have been approved for marketing on the basis of showing a survival advantage. Many of our existing and potential competitors have substantially greater financial resources and expertise than we do in manufacturing and developing products, conducting clinical trials, obtaining regulatory approvals and marketing. These entities also compete with us in recruiting and retaining qualified scientific and management personnel, as well as in acquiring products and technologies complementary to our programs. Standard treatments vary considerably by cancer indication, and new drugs may be more effective in treating one cancer indication than another. In addition, cancer is a difficult disease to treat and it is likely that no one therapeutic will replace all other therapies in any particular indication. Therapeutic strategies for treating cancer are increasingly focused on combining a number of drugs in order to yield the best results. Since custirsen and apatorsen are intended to be used in multiple cancer indications and target the tumors’ adaptive survival mechanisms, these drugs may potentially be synergistic with many new and currently marketed therapies. Our ability to compete successfully will depend largely on our ability and, where applicable, the ability of our collaborators to:
|
|
· |
maintain or establish development programs in combination with new agents that may replace or diminish the markets for which we are currently developing our product candidates; |
|
|
· |
establish that our product candidates are well tolerated and result in a clinical benefit when administered to cancer patients; |
|
|
· |
establish that our product candidates address significant unmet needs for patients, resulting in prioritization of our product candidates over other treatment options; |
|
|
· |
advance the development of our lead programs, including the enrollment of patients for our clinical trials; |
|
|
· |
gain regulatory approval for our product candidates in their respective first indications as well as expand into additional indications; |
|
|
· |
commercialize our lead product candidates successfully, which includes convincing physicians, insurers and other third-party payors of the advantages of our products over current therapies, when and if they have advantages; |
|
|
· |
obtain intellectual property protection and protect the exclusivity for our product candidates and products, when and if we have any; and |
|
|
· |
acquire other product candidates to expand our pipeline. |
EMPLOYEES
As of December 31, 2015, we had a total of 41 employees, of whom 23 were engaged in research and development functions, including clinical development, regulatory affairs and manufacturing, and 18 were engaged in general and administrative functions, including accounting and finance, administration, and corporate communications. In February 2016, we announced a plan to reduce operating expenses, which included a workforce reduction of 11 employees.
All of our employees have entered into non-disclosure agreements regarding our intellectual property, trade secrets and other confidential information. None of our employees are represented by a labor union or covered by a collective bargaining agreement, nor have we experienced any work stoppages. We believe that we maintain satisfactory relations with our employees.
From time to time, we also use outside consultants to provide advice on our clinical development plans, research programs, administration and potential acquisitions of new technologies.
FINANCIAL INFORMATION
We manage our operations and allocate resources as a single reporting segment. Financial information regarding our operations, assets and liabilities, including our total revenue and net loss for the years ended December 31, 2015, 2014 and 2013 and our total assets as of December 31, 2015 and 2014, is included in our Consolidated Financial Statements in Part II, Item 8 of this Annual Report on Form 10-K.
24
COMPANY INFORMATION
We were incorporated in California in October 1991 and subsequently reorganized as a Delaware corporation in March 1995. Our principal executive offices are located at 19820 North Creek Parkway, Bothell Washington 98011, and our telephone number is (425) 686-1500.
In August 2008, our company, then named Sonus Pharmaceuticals, Inc., completed its acquisition, or the Arrangement, of OncoGenex Technologies, a Canadian corporation, as contemplated by the Arrangement Agreement between the companies. We then changed our name to OncoGenex Pharmaceuticals, Inc. As a result of the Arrangement, OncoGenex Technologies became our wholly owned subsidiary. OncoGenex Technologies was incorporated under the federal laws of Canada in May 2000. OncoGenex, Inc., a former subsidiary of OncoGenex Technologies, was incorporated under the laws of Washington in August 2005 and was dissolved pursuant to the Articles of Dissolution filed on July 1, 2009. As used in this Annual Report on Form 10-K, the term “Sonus” refers to our business prior to August 21, 2008.
AVAILABLE INFORMATION
We maintain a website at http://www.oncogenex.com. The information contained on or accessible through our website is not part of this Annual Report on Form 10-K. Our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and amendments to reports filed or furnished pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended, or Exchange Act, are available free of charge on our website as soon as reasonably practicable after we electronically file such reports with, or furnish those reports to, the SEC. Any information we filed with the SEC may be accessed and copied at the SEC’s Public Reference Room at 100 F Street NE, Washington, DC 20549. Information may be obtained by calling the SEC at 1-800-SEC-0330. The SEC also maintains an Internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC at http://www.sec.gov.
Risks Related to Our Business
Investing in our common stock involves a high degree of risk. You should consider carefully the risks and uncertainties described below, together with all of the other information contained in this Annual Report on Form 10-K and in the other periodic and current reports and other documents we file with the Securities and Exchange Commission, before deciding to invest in our common stock. If any of the following risks materialize, our business, financial condition, results of operation and future prospects will likely be materially and adversely affected. In that event, the market price of our common stock could decline and you could lose all or part of your investment.
Risks Related to Our Business
We have incurred losses since inception and anticipate that we will continue to incur losses for the foreseeable future. We have never had any products available for commercial sale and we may never achieve or sustain profitability.
We are a clinical-stage biopharmaceutical company, are not profitable, have incurred losses in each year since our inception and do not expect to become profitable in the foreseeable future. We have never had any products available for commercial sale, and we have not generated any revenue from product sales nor do we anticipate that we will generate revenue from product sales in the near future. Our revenue to date has been collaboration revenue under the Collaboration Agreement with Teva, which was terminated in April 2015. As a result of the termination of the Collaboration Agreement, Teva will no longer be responsible for custirsen-related expenses, and we will not receive additional revenue from Teva other than the advanced reimbursement payment for custirsen-related expenses we received in connection with the termination of the Collaboration Agreement. We have not yet submitted any products for approval by regulatory authorities, and we continue to incur research and development and general and administrative expenses related to our operations. We expect to continue to incur losses for the foreseeable future, and we expect these losses to increase as we continue our research activities and conduct development of, and seek regulatory approvals for, our product candidates, and prepare for and begin to commercialize any approved products. If our product candidates fail in clinical trials or do not gain regulatory approval, or if our product candidates do not achieve market acceptance, we may never become profitable. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods.
Clinical trials may not demonstrate a clinical benefit of our product candidates.
Positive results from preclinical studies and clinical trials, including any exploratory results from the custirsen or apatorsen clinical trials conducted to date should not be relied on as evidence that on-going, amended, or later-stage or large-scale clinical trials will succeed. We will be required to demonstrate with substantial evidence through well-controlled clinical trials that our product candidates are safe and effective for use in a diverse population before we can seek regulatory approvals for their commercial sale.
25
Success in early clinical trials does not mean that future clinical trials will be successful because product candidates in later-stage clinical trials may fail to demonstrate sufficient safety and efficacy to the satisfaction of regulatory agencies, despite having progressed through initial clinical trials. Further, preliminary results from our clinical trials may not be confirmed in final data, or may change materially.
Even after the completion of our planned Phase 3 clinical trials, regulatory agencies may disagree with our clinical trial design and our interpretation of data, and may require us to conduct additional clinical trials to demonstrate the efficacy of our product candidates.
We have amended some of our ongoing clinical trials to incorporate preliminary observations from our other completed clinical trials. These observations may not be applicable to other stages of disease, or in combination with other therapies or indications. In planning or completing amendments to our trials, the statistical requirements to demonstrate success have been increased. This is due to including fewer patients for the primary evaluation and/or due to allowing for the chance of success to be determined in either of two primary evaluations, rather than only having one primary evaluation specified. Accordingly, if the observations from other completed trials are applied as amendments to our ongoing trials but prove not to be applicable to our ongoing trials, the results might indicate that our original trial design would have been successful if the changes had not been made to the original statistical requirements. We may choose to make additional amendments to ongoing studies for any reason including to analyze final top line data earlier than planned. Any future amendments may compromise the integrity of the clinical trial results and may not be acceptable to regulators.
We are highly dependent on the success of our lead product candidates, custirsen and apatorsen, and we cannot give any assurance that they, or any of our other product candidates, will receive regulatory approval or will be successfully commercialized.
In order to market custirsen, we must, among other things, complete ongoing clinical trials, including phase 3 or registration clinical trials, to demonstrate safety and efficacy. In April 2014, we announced that top-line survival results from our phase 3 SYNERGY trial indicated that the addition of custirsen to standard first-line docetaxel/prednisone therapy did not meet the primary endpoint of a statistically significant improvement in overall survival in men with metastatic CRPC, compared to docetaxel/prednisone alone. Our protocol amendments, including but not limited to revisions to statistical analysis plans, or inclusion of analyses on poor prognostic patients, may be approved by regulatory authorities on a country-by-country basis slower than we anticipate, or not at all. We may decide not to continue to advance the development and commercialization of custirsen, which would harm or prevent the commercialization of this product candidate. The failure to further develop and eventually commercialize custirsen could have a material adverse effect on our business and financial condition.
Completing additional clinical trials will be required for apatorsen to establish the safety and efficacy of this product candidate. In September 2015, we announced that the addition of apatorsen to ABRAXANE and gemcitabine did not demonstrate a survival benefit compared to ABRAXANE and gemcitabine alone. Additionally, in January 2016, we announced that data from the phase 2 Spruce trial evaluating the combination of apatorsen with carboplatin and pemetrexed in patients with untreated metastatic NSCLC did not reach the statistical significance required to demonstrate a PFS benefit. We are conducting parallel clinical trials to evaluate apatorsen in several cancer indications and treatment combinations. The failure of apatorsen to be shown safe or effective in one or more indications could negatively impact the development of apatorsen in other indications and could result in the suspension or termination of our apatorsen development plans.
OGX-225 has not been tested in humans. Our preclinical testing of this product candidate may not be favorable and we may not be able to clinically evaluate OGX-225.
Our clinical development programs for our product candidates may not receive regulatory approval either if such product candidates fail to demonstrate that they are safe and effective in clinical trials and consequently fail to obtain necessary approvals from the regulatory agencies, or if we have inadequate financial or other resources to advance these product candidates through the clinical trial process. If competitive products developed by third parties show significant benefit in the cancer indications in which we are developing our product candidates, any planned supportive or primary registration trials may be delayed, altered or not initiated and custirsen, apatorsen and our other product candidates may never receive regulatory approval. Any failure to obtain regulatory approval of custirsen, apatorsen or our other product candidates could have a material and adverse effect on our business.
26
We rely on third parties to manufacture and supply our product candidates and other agents used in our clinical trials and potential future commercial use. A decrease in the availability or quality of any of these products or agents could increase clinical trial costs, delay or halt clinical development or regulatory approval of our product candidates or commercialization of our future product candidates, resulting in additional losses and depriving us of potential product revenue.
We do not own or operate manufacturing facilities, and we depend on third-party contract manufacturers for production of all of our product candidates and rely on other companies and their manufacturers for other agents used in all of our clinical trials. We lack the resources and the capability to manufacture any of our product candidates ourselves. To date, our product candidates have been manufactured in limited quantities for preclinical studies and clinical trials. All active pharmaceutical ingredients, or API, and drug product for custirsen and apatorsen have been manufactured for us by third parties pursuant to a purchase order or short-term contract that has been fulfilled.
Prior to the termination of our collaboration agreement with Teva, Teva manufactured custirsen drug product and, pursuant to the Termination Agreement, it has discontinued such activities. In addition to the selection of a new drug product supplier, we will require technology and methods transfer, validation processes and stability data in order to manufacture drug product. These activities, results and associated regulatory requirements may delay our ability to submit our application for market approval, if applicable. We cannot provide assurance that we will find a new manufacturer of drug product whose terms or timing would be acceptable to us and we may not have sufficient resources to commence certain activities as soon as required. As a result, we could experience a significant delays in custirsen’s development and potential future commercialization.
If, in the future, one of our product candidates is approved for commercial sale, we, or a pharmaceutical partner that has licensed such product candidate, may need to manufacture that product candidate in commercial quantities. We cannot provide assurance that the third-party manufacturers with which we have contracted in the past will have sufficient capacity to satisfy our future manufacturing needs, that we will be able to negotiate additional purchases of API or drug product from these or alternative manufacturers on terms favorable to us, if at all, or that a pharmaceutical partner that has licensed such product candidate will have sufficient capacity or expertise to satisfy future needs.
Third-party manufacturers may fail to perform under their contractual obligations, or may fail to deliver the required commercial quantities of bulk API or finished drug product on a timely basis and at commercially reasonable prices. We have experienced manufacturing quality issues resulting in an unusable lot of product candidate in the past. Any performance failure on the part of our contract manufacturers could delay clinical development or regulatory approval of our product candidates or commercialization of our future product candidates, depriving us of potential product revenue and resulting in additional losses. If we are required to identify and qualify an alternate manufacturer, we may be forced to delay or suspend our clinical trials, regulatory submissions, required approvals or commercialization of our product candidates, which may cause us to incur higher costs and could prevent us from commercializing our product candidates successfully. If we are unable to find one or more replacement manufacturers capable of production at a reasonably favorable cost, in adequate volumes, of adequate quality and on a timely basis, we would likely be unable to meet demand for our product candidates and our clinical trials could be delayed or we could lose potential revenue. Our ability to replace an existing API manufacturer may be difficult because the number of potential manufacturers is limited to approximately five manufacturers, and regulatory agencies must inspect any replacement manufacturer and review information related to product produced at the manufacturer before they can begin manufacturing our product candidates. It may be difficult or impossible for us to identify and engage a replacement manufacturer on acceptable terms in a timely manner, if at all. We expect to continue to depend on third-party contract manufacturers for the foreseeable future.
Our product candidates require precise, high-quality manufacturing. Any of our contract manufacturers will be subject to ongoing periodic unannounced inspection by regulatory agencies to ensure strict compliance with current Good Manufacturing Practices, or cGMP, and other applicable government regulations and corresponding standards. If our contract manufacturers fail to achieve and maintain high manufacturing standards in compliance with cGMP regulations, we may experience manufacturing errors resulting in patient injury or death, product recalls or withdrawals, delays or interruptions of production or failures in product testing or delivery, delay or prevention of filing or approval of marketing applications for our product candidates, cost overruns or other problems that could seriously affect our business.
Significant manufacturing scale-up may require additional validation studies, which the regulatory agencies must review and approve. Additionally, any third-party manufacturers we retain to manufacture our product candidates on a commercial scale must pass regulatory agencies’ pre-approval inspection for conformance to cGMP regulations before we can obtain approval of our product candidates. If we are unable to successfully increase the manufacturing capacity for a product candidate in conformance with cGMP regulations, the regulatory approval or commercial launch of any related products may be delayed or there may be a shortage in supply.
We also rely on third-parties for the provision of other agents used in our clinical trials, and in some circumstances these agents are provided to us at no cost. We have no assurance that these third-parties will continue to provide their products to us at no cost.
27
The termination of our Collaboration Agreement with Teva has resulted in us being required to take over responsibility for conducting the ongoing custirsen trials, and further development and commercialization of custirsen will require significant resources from us or another collaborator.
In April 2015, we and Teva entered into a Termination Agreement, pursuant to which we terminated our Collaboration Agreement. Under the terms of the Termination Agreement, we received approximately $23.2 million as advanced reimbursement for custirsen-related development activities and regained all rights to custirsen and responsibility for all custirsen-related expenses as of January 1, 2015, including those related to the ENSPIRIT trial, as well as manufacturing and regulatory activities for the custirsen programs, which were previously managed and funded by Teva. Of the advance reimbursement received, we have incurred approximately $18.2 million for certain custirsen-related development costs between January 1, 2015 and December 31, 2015. As a result, Teva transitioned the responsibilities associated with conducting the ongoing custirsen clinical trials to us.
Additionally, further development of custirsen will require significant resources from us or another collaborator. We will not receive any future cash reimbursements from Teva for costs incurred by us in connection with the clinical development of custirsen, and we are required to fund all future development and commercialization ourselves if we are unable to find another collaborator. We expect that the $23.2 million payment from Teva as advanced reimbursement for custirsen-related development activities, along with our existing capital resources, will allow for the completion and final results from the AFFINITY and ENSPIRIT trials, but we will need to acquire additional capital or enter into a new partnership or collaboration agreement to fund additional development or commercialization. There are no assurances that we will have access to additional capital or find a new collaborator, or that the terms and timing of any such arrangements would be acceptable to us. As a result, we could experience a significant delay in the custirsen development process. If we determine to discontinue the development of custirsen, or any ongoing clinical trials, we would not receive any future return on our investment from that product candidate, or a specific indication.
Because we depend on financing from third parties for our operations, our business may fail if such financing becomes unavailable or is not available on commercially reasonable terms.
To date, we have financed our operations primarily through the sale of our equity securities and from payments we received pursuant to the Collaboration Agreement with Teva. In April 2015, our Collaboration Agreement with Teva was terminated, and we will not receive any future payments from Teva. We believe that our existing capital resources and interest on such resources will be sufficient to meet our current operating requirements into the third quarter of 2017. However, if patients live longer as a result of new or investigational therapies, the trials proceed slower or take longer than expected to complete, or are initiated later than expected, we change our development plans, acquire rights to new product candidates, cannot find third-party collaborators for our other product candidates, do not successfully defend pending litigation or engage in commercialization and product launch activities, we will need additional capital sooner than we expect. Our future capital requirements will depend on many factors, including, without limitation:
|
|
· |
the scope and results of our clinical trials and preclinical studies; |
|
|
· |
whether we experience delays in our clinical and preclinical development programs, or experience slower-than-anticipated product development or rate of events; |
|
|
· |
whether we are able to enter into additional third-party collaborative partnerships to develop and/or commercialize any of our other product candidates on terms that are acceptable to us; |
|
|
· |
our ability to forecast the cost of our ongoing development activities, including the ENSPIRIT trial; |
|
|
· |
the timing and requirements of, and the costs involved in, making protocol amendments to any of our ongoing studies prior to their completion and conducting studies required to obtain regulatory approvals for our product candidates from regulatory agencies; |
|
|
· |
the availability of third parties to perform the key development tasks for our product candidates, including conducting preclinical studies and clinical trials and manufacturing our product candidates to be tested in those studies and trials and the associated costs of those services; |
|
|
· |
the costs involved in preparing, filing, prosecuting, maintaining, defending the validity of and enforcing patent claims and other costs related to patent rights and other intellectual property rights, including litigation costs and the results of such litigation; |
|
|
· |
whether we modify our development program, including terminating and starting new trials; |
|
|
· |
whether opportunities to acquire additional product candidates arise and the costs of acquiring and developing those product candidates; |
|
|
· |
whether we engage in commercialization and product launch activities; and |
|
|
· |
the costs to defend, and the results of, pending litigation. |
28
If we are unable to raise funds on acceptable terms when it becomes necessary to do so, we may not be able to continue developing our product candidates, acquire or develop additional product candidates or respond to competitive pressures or unanticipated requirements. For these reasons, any inability to raise additional funds when we require it could have a material adverse effect on our business.
We may fail to achieve the expected financial and operating benefits of our plan to reduce operating expenses and the plan may harm our business and financial results.
In February 2016, we announced a plan to reduce operating expenses, which included a workforce reduction of 11 employees, representing approximately 27% of our employees prior to the reduction. We face significant risks associated with this plan that may impair our ability to achieve anticipated savings and operational efficiencies or that may otherwise harm our business. These risks include delays in implementation of anticipated workforce reductions, loss of workforce capabilities, decreases in employee focus and morale, attrition of necessary or key employees, higher than anticipated separation expenses, litigation and the failure to meet financial and operational targets. In addition, the calculation of the anticipated cost savings and other benefits resulting from our plan to reduce operating expenses are subject to many estimates and assumptions. These estimates and assumptions are subject to significant business, economic, competitive and other uncertainties and contingencies, many of which are beyond our control. If these estimates and assumptions are incorrect or if we experience delays or unforeseen events, our business and financial results could be adversely affected.
We rely, in part, on third parties to conduct clinical trials for our product candidates and plan to rely on third parties to conduct future clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may be unable to obtain regulatory approval for or commercialize our current and future product candidates.
To implement our product development strategies, we rely on third parties, such as collaborators, contract research organizations, medical institutions, clinical investigators and contract laboratories, to conduct clinical trials of our product candidates. Although we rely on third parties to conduct our clinical trials, we are responsible for ensuring that each of our clinical trials is conducted in accordance with our development plan and protocol. Moreover, regulatory agencies require us to comply with regulations and standards, commonly referred to as Good Clinical Practices, or GCPs, for conducting, monitoring, recording and reporting the results of clinical trials to ensure that the data and results are scientifically credible and accurate and that the clinical trial subjects are adequately informed of the potential risks of participating in clinical trials. Our reliance on third parties does not relieve us of these responsibilities and requirements. If the third parties conducting our clinical trials do not perform their contractual duties or obligations, do not meet expected deadlines or need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to GCPs or for any other reason, we may need to enter into new arrangements with alternative third parties and our clinical trials may be extended, delayed or terminated. In addition, a failure by such third parties to perform their obligations in compliance with GCPs may cause our clinical trials to fail to meet regulatory requirements, which may require us to repeat our clinical trials.
Our clinical trials may be suspended or terminated at any time, including by regulatory agencies, a Data Safety Monitoring Board overseeing the clinical trial at issue, by a clinical trial site or investigator, or by us. Any failure or significant delay in completing clinical trials for our product candidates could materially harm our financial results and the commercial prospects for our product candidates.
We do not know whether any of our currently planned or on-going clinical trials for custirsen or apatorsen will proceed or be completed on schedule, if at all, or, with respect to our other product candidates, whether we will be able to initiate any future preclinical studies or clinical trials, as applicable, beyond those currently planned. The completion of our clinical trials currently in progress could also be substantially delayed or prevented by several factors, including:
|
|
· |
delay or failure to obtain required future additional funding, when needed, through private or public offerings of our equity securities, debt financings, or the execution of a licensing, partnership or collaboration agreement with a third party for any of our product candidates; |
|
|
· |
lack of efficacy evidenced during clinical trials; |
|
|
· |
inadequate evidence of clinical benefit or futility; |
|
|
· |
slower than expected rates of patient recruitment, enrollment and final analysis; |
|
|
· |
failure of patients to complete the clinical trial; |
|
|
· |
unforeseen safety issues; |
|
|
· |
termination of our clinical trials by one or more clinical trial sites, investigators, data safety monitoring boards, or regulatory agencies; |
29
|
|
· |
inability or unwillingness of patients or medical investigators to follow clinical trial protocols; |
|
|
· |
inability to monitor patients adequately during or after treatment; |
|
|
· |
introduction of competitive products that may impede our ability to retain patients in clinical trials; |
|
|
· |
delay or failure to obtain sufficient manufacturing supply of custirsen or apatorsen; and |
|
|
· |
delay in submission or acceptance of protocol amendments. |
The completion or commencement of future preclinical studies or clinical trials could be substantially delayed or prevented by several factors, including:
|
|
· |
delay or failure to obtain required future additional funding, when needed, through private or public offerings of our equity securities, debt financings, or the execution of a licensing, partnership or collaboration agreement with a third party for any of our product candidates; |
|
|
· |
delay or failure to obtain sufficient manufacturing supply of custirsen, apatorsen or other products necessary to conduct our clinical trials; |
|
|
· |
limited number of, and competition for, suitable patients with the particular types of cancer required for enrollment in our clinical trials; |
|
|
· |
limited number of, and competition for, suitable sites to conduct clinical trials; |
|
|
· |
introduction of new product candidates to the market in therapeutic areas similar to those that we are developing for our product candidates; |
|
|
· |
concurrent evaluation of new investigational product candidates in therapeutic areas similar to those that we are developing for our product candidates; |
|
|
· |
delay or failure to obtain regulatory agencies’ approval or agreement to commence a clinical trial, including our phase 3 or registration clinical trials or amendment of those trials; |
|
|
· |
delay or failure to obtain sufficient supplies, including comparator drug, for our clinical trials; delay or failure to reach agreement on acceptable clinical trial agreement terms or clinical trial protocols with prospective sites or investigators; |
|
|
· |
delay or failure to obtain the approval of the Institutional Review Board to conduct a clinical trial at a prospective site; and |
|
|
· |
our decision to alter the development strategy for one or more clinical or preclinical products. |
We may seek to partner with third-party collaborators with respect to the development and commercialization of our product candidates, and we cannot control whether we will be able to do so on favorable terms, if at all.
Our business strategy relies in part on potentially partnering successful product candidates with larger companies to complement our internal development and commercialization efforts. We will be competing with many other companies as we seek partners for our product candidates and may not be able to compete successfully against those companies. If we are not able to enter into collaboration arrangements for our product candidates, we would be required to undertake and fund further development, clinical trials, manufacturing and commercialization activities solely at our own expense and risk. If we are unable to finance and/or successfully execute those expensive activities, or we delay such activities due to capital availability, our business could be materially and adversely affected, and potential future product launch could be materially delayed, be less successful, or we may be forced to discontinue clinical development of these product candidates.
Our product candidates may cause undesirable and potentially serious side effects during clinical trials that could delay or prevent their regulatory approval or commercialization.
Since patients in our clinical trials have advanced stages of cancer, we expect that additional adverse events, including serious adverse events, will occur.
30
Undesirable side effects caused by any of our product candidates could cause us or regulatory authorities to interrupt, delay or halt clinical trials and could result in the denial of regulatory approval by regulatory agencies for any or all targeted indications or decrease the competitive opportunity of the product candidate which may decrease sales potential. This, in turn, could prevent us from commercializing our product candidates and generating revenue from their sale. In addition, if our product candidates receive marketing approval and we or others later identify undesirable side effects caused by the product:
|
|
· |
we may elect to terminate the ongoing clinical trials and cease development of the product; |
|
|
· |
regulatory authorities may withdraw their approval of the product; |
|
|
· |
we may be required to recall the product, change the way the product is administered, conduct additional clinical trials or change the labeling of the product; |
|
|
· |
a product may become less competitive and product sales may decrease; and |
|
|
· |
our reputation may suffer. |
Any one or a combination of these events could prevent us from achieving or maintaining market acceptance of the affected product or could substantially increase the costs and expenses of commercializing the product, which in turn could delay or prevent us from generating significant revenue from the sale of the product. Historic events have raised questions about the safety of marketed drugs and may result in increased cautiousness by regulatory agencies in reviewing new drugs based on safety, efficacy or other regulatory considerations and may result in significant delays in obtaining regulatory approvals, additional clinical trials being required, or more stringent product labeling requirements. Any delay in obtaining, or the inability to obtain, applicable regulatory approvals would prevent us from commercializing our product candidates.
If we were to be successfully sued related to our products or operations, we could face substantial liabilities that may exceed our resources.
We may be held liable if any of our products or operations cause injury or death or are found otherwise unsuitable during product testing, manufacturing, marketing or sale. These risks are inherent in the development of pharmaceutical products. We currently maintain commercial general and umbrella liability policies with combined limits of $10.0 million per occurrence and in the aggregate, in addition to a $10.0 million per claim and annual aggregate product liability insurance policy related to our clinical trials consistent with industry standards. When necessary for our products, we intend to obtain additional product liability insurance. Insurance coverage may be prohibitively expensive, may not fully cover potential liabilities or may not be available in the future. Inability to obtain sufficient insurance coverage at an acceptable cost or otherwise to protect against potential product liability claims could prevent or inhibit the commercialization of our products. If we were to be sued for any injury caused by or associated with our products or operations, the litigation could consume substantial time and attention of our management, and the resulting liability could exceed our total assets.
If our competitors develop and market products that are more effective, safer or less expensive than our future product candidates, our clinical trials and commercial opportunities will be negatively affected.
The life sciences industry is highly competitive, and we face significant competition from many pharmaceutical, biopharmaceutical and biotechnology companies that are researching and marketing products designed to address cancer indications for which we are currently developing products or for which we may develop products in the future. We are aware of several other companies that are developing therapeutics that seek to promote tumor cell death. Several therapies have been recently approved by the FDA, and we expect more to be approved in the future.
Some of our product candidates’ development plans include pursuing prostate and lung cancer indications. Substantial advancements in the treatment of prostate and lung cancer have occurred in the past two years and new products from our competitors have been approved for marketing on the basis of showing a survival advantage. Any products we may develop in the future are also likely to face competition from other drugs and therapies. Many of our competitors have significantly greater financial, manufacturing, marketing and drug development resources than we do. Large pharmaceutical companies, in particular, have extensive experience in clinical testing and in obtaining regulatory approvals for drugs. These companies also have significantly greater research and marketing capabilities than we do. In addition, many universities and private and public research institutes are, or may become, active in cancer research, and develop products that may directly compete with ours. If our competitors market products that are more effective, safer or less expensive than our future product candidates, if any, or that reach the market sooner than our future product candidates, if any, we may not achieve commercial success.
31
If new therapies become broadly used, we may need to conduct clinical trials of our product candidates in combination with these new therapies to demonstrate safety and efficacy of the combination. Additional trials will delay the development of our product candidates and increase our costs. The failure of certain of our product candidates to work in combination with these new therapies would have an adverse effect on our business.
Our intention is to combine certain of our product candidates with therapies that are broadly used by clinicians and considered highly effective. As new therapies are developed, we will need to assess these therapies to determine whether to conduct clinical trials of our product candidates in combination with them to demonstrate safety and efficacy of the combination. If we determine that it is appropriate to conduct additional clinical trials of our product candidates in combination with these new therapies, the development of our product candidates will be delayed and our costs will be increased. If these clinical trials generate safety concerns or lack of efficacy, our business would be adversely affected.
Even if we receive regulatory approval to market our product candidates, the market may not be receptive to our products.
Even if our product candidates obtain regulatory approval, they may not gain market acceptance among physicians, patients, healthcare payors and/or the medical community. We believe that the degree of market acceptance will depend on a number of factors, including:
|
|
· |
timing of market introduction of competitive products; |
|
|
· |
safety and efficacy of our products; |
|
|
· |
prevalence and severity of any side effects; |
|
|
· |
potential advantages or disadvantages over alternative treatments; |
|
|
· |
strength of marketing and distribution support; |
|
|
· |
price of our products, both in absolute terms and relative to alternative treatments; |
|
|
· |
availability of coverage and reimbursement from government and other third-party payors; and |
|
|
· |
sequencing of available products. |
If our future product candidates fail to achieve market acceptance, we may not be able to generate significant revenue or achieve or sustain profitability.
We will need to retain additional personnel and expand our other resources in order to develop our other product candidates. If we fail to effectively expand our operations, including attracting and retaining key management and scientific personnel, we may be unable to successfully develop or commercialize our product candidates and our business may be materially adversely affected.
We will need to expand and effectively manage our managerial, operational, financial, development, commercialization and other resources in order to successfully pursue our development and commercialization efforts for our existing and future product candidates. In connection with the termination of the Collaboration Agreement with Teva, we took on additional management activities such as regulatory, drug supply and pharmacovigilance that was previously managed by Teva. Our success depends on our continued ability to attract, retain and motivate highly qualified personnel, such as management, clinical and preclinical personnel, including our executive officers Scott Cormack, John Bencich and Cindy Jacobs. In addition, although we have entered into employment agreements with each of Mr. Cormack, Mr. Bencich and Dr. Jacobs, such agreements permit the executive to terminate his or her employment with us at any time, subject to providing us with advance written notice.
Should custirsen receive marketing approval in the United States, Canada, or elsewhere in the world, we would need to hire a substantial number of specialized personnel, including field-based medical affairs representatives. In turn, we would need to increase our administrative headcount to support such expanded development and commercialization operations with respect to our product candidates. Our ability to attract and retain qualified personnel in the future is subject to intense competition for qualified personnel among biotechnology, pharmaceutical and other businesses and our current financial position. The loss of the services of any of our senior management could delay or prevent the development and commercialization of our product candidates, or have other adverse effects on our business for an indefinite term. In particular, if we lose any members of our current senior management team, we may not be able to find suitable replacements in a timely fashion, if at all, and our business may be harmed as a result.
We have scientific and clinical advisors who assist us in formulating our development and clinical strategies. These advisors are not our employees and may have commitments to, or consulting or advisory contracts with, other entities that may limit their availability to us. In addition, our advisors may have arrangements with other companies to assist those companies in developing products or technologies that may compete with ours.
32
We may encounter difficulties in managing our expected growth and in expanding our operations successfully.
As we advance our product candidates through development, we will need to develop or expand our development, regulatory, manufacturing, marketing and sales capabilities or contract with third parties to provide these capabilities for us. Maintaining additional relationships and managing our future growth will impose significant added responsibilities on members of our management. We must be able to manage our development efforts effectively, manage our clinical trials effectively, hire, train and integrate additional management, development, administrative and sales and marketing personnel, improve our managerial, development, operational and finance systems, and expand our facilities, all of which may impose a strain on our administrative and operational infrastructure.
Furthermore, we may acquire additional businesses, products or product candidates that complement or augment our existing business. Integrating any newly acquired business, product or product candidate could be expensive and time-consuming. We may not be able to integrate any acquired business, product or product candidate successfully or operate any acquired business profitably. Our future financial performance will depend, in part, on our ability to manage any future growth effectively and our ability to integrate any acquired businesses. We may not be able to accomplish these tasks, which failure could prevent us from successfully growing our business.
If we fail to acquire and develop products or product candidates at all or on commercially reasonable terms, we may be unable to grow our business.
We currently do not have internal discovery capabilities and depend on pharmaceutical and biotechnology companies and other researchers to sell or license products or product candidates to us. To date, three of our product candidates have been derived from technologies discovered by the Vancouver Prostate Centre and licensed to us by UBC. We intend to continue to rely on research institutions and other biotechnology or pharmaceutical companies as sources of product candidates. We cannot guarantee that the Vancouver Prostate Centre or UBC will continue to develop new product candidate opportunities, that we will continue to have access to such opportunities or that we will be able to purchase or license these product candidates on commercially reasonable terms, if at all. If we are unable to purchase or license new product candidates from the Vancouver Prostate Centre or UBC, we will be required to identify alternative sources of product candidates.
The success of our product pipeline strategy depends on our ability to identify, select and acquire pharmaceutical product candidates. Proposing, negotiating and implementing an economically viable product acquisition or license is a lengthy and complex process. We compete for partnering arrangements and license agreements with pharmaceutical and biotechnology companies and academic research institutions. Our competitors may have stronger relationships with third parties with whom we are interested in collaborating and/or may have more established histories of developing and commercializing products. As a result, our competitors may have a competitive advantage in entering into partnering arrangements with such third parties. In addition, even if we find promising product candidates, and generate interest in a partnering or strategic arrangement to acquire such product candidates, we may not be able to acquire rights to additional product candidates or approved products on terms that we find acceptable, if at all. If we fail to acquire and develop product candidates from others, we may be unable to grow our business.
We expect that any product candidate that we acquire rights to will require additional development efforts prior to commercial sale, including extensive clinical evaluation and approval by regulatory agencies. All product candidates are subject to the risks of failure inherent in pharmaceutical product development, including the possibility that the product candidate will not be shown to be sufficiently safe and effective for approval by regulatory authorities. Even if the product candidates are approved, we can make no assurance that we would be capable of economically producing the product or that the product would be commercially successful.
We may be adversely affected if our controls over financial reporting fail or are circumvented.
We regularly review and update our internal controls, disclosure controls and procedures, and corporate governance policies. In addition, we are required under the Sarbanes Oxley Act of 2002 to report annually on our internal control over financial reporting. If it were to be determined that our internal control over financial reporting is not effective, such shortcoming could have an adverse effect on our business and financial results and the price of our common stock could be negatively affected. This reporting requirement could also make it more difficult or more costly for us to obtain certain types of insurance, including director and officer liability insurance, and we may be forced to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. Any system of internal controls, however well designed and operated, is based in part on certain assumptions and can provide only reasonable, not absolute, assurances that the objectives of the system are met. Any failure or circumvention of the controls and procedures or failure to comply with regulation concerning control and procedures could have a material effect on our business, results of operation and financial condition. Any of these events could result in an adverse reaction in the financial marketplace due to a loss of investor confidence in the reliability of our financial statements, which ultimately could negatively affect the market price of our shares, increase the volatility of our stock price and adversely affect our ability to raise additional funding. The effect of these events could also make it more difficult for us to attract and retain qualified persons to serve on our Board and our Board committees and as executive officers.
33
Risks Related to Our Intellectual Property
Our proprietary rights may not adequately protect our technologies and product candidates.
Our commercial success will depend on our ability to obtain patents and/or regulatory exclusivity and maintain adequate protection for our technologies and product candidates in the United States and other countries. We will be able to protect our proprietary rights from unauthorized use by third parties only to the extent that our proprietary technologies and future product candidates are covered by valid and enforceable patents or are effectively maintained as trade secrets.
We and our collaborators intend to apply for additional patents covering both our technologies and product candidates, as we deem appropriate. We or our collaborators may, however, fail to apply for patents on important technologies or product candidates in a timely fashion, if at all. Our existing patents and any future patents we or our collaborators obtain may not be sufficiently broad to prevent others from practicing our technologies or from developing competing products and technologies. In addition, we do not always control the patent prosecution of subject matter that we license from others. Accordingly, we are sometimes unable to exercise a significant degree of control over such intellectual property as we would over our own.
Moreover, the patent positions of biopharmaceutical companies are highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. As a result, the validity and enforceability of our patents cannot be predicted with certainty. In addition, the U.S. Supreme Court has revised certain tests regarding granting patents and assessing the validity of patents to make it more difficult to obtain patents. As a consequence, issued patents may be found to contain invalid claims according to the revised standards. Some of our patents or those of our collaborators may be subject to challenge and subsequent invalidation or significant narrowing of claim scope in a re-examination proceeding, or during litigation, under the revised criteria. We cannot guarantee that:
|
|
· |
we or our licensors were the first to make the inventions covered by each of our issued patents and pending patent applications; |
|
|
· |
we or our licensors were the first to file patent applications for these inventions; |
|
|
· |
others will not independently develop similar or alternative technologies or duplicate any of our technologies; |
|
|
· |
any of our or our licensors’ pending patent applications will result in issued patents; |
|
|
· |
any of our or our licensors’ patents will be valid or enforceable; |
|
|
· |
any patents issued to us or our licensors and collaboration partners will provide us with any competitive advantages, or will not be challenged by third parties; and |
|
|
· |
we will develop additional proprietary technologies that are patentable, or the patents of others will not have an adverse effect on our business. |
The actual protection afforded by a patent varies on a product-by-product basis, from country to country and depends on many factors, including the type of patent, the scope of its coverage, the availability of regulatory related extensions, the availability of legal remedies in a particular country and the validity and enforceability of the patents. Our ability or the ability of our collaborators to maintain and solidify our proprietary position for our product candidates will depend on our success in obtaining effective claims and enforcing those claims once granted. Our issued patents and those that may issue in the future, or those licensed to us or our collaborators, may be challenged, invalidated, unenforceable or circumvented, and the rights granted under any issued patents may not provide us with proprietary protection or competitive advantages against competitors with similar products. Due to the extensive amount of time required for the development, testing and regulatory review of a potential product, it is possible that, before any of our product candidates can be commercialized, any related patent may expire or remain in force for only a short period following commercialization, thereby reducing any advantage of the patent.
We also rely on trade secrets to protect some of our technology, especially where it is believed that patent protection is not appropriate or obtainable. However, trade secrets are difficult to maintain. While we use reasonable efforts to protect our trade secrets, our or our collaboration partners’ employees, consultants, contractors or scientific and other advisors may unintentionally or willfully disclose our proprietary information to competitors. For example, under our Termination Agreement with Teva, Teva is not permitted to use our confidential information which would include our trade secrets. We may not be able to adequately determine whether Teva uses any of our trade secrets and if they do, we may not be able to sufficiently enforce their non-use. Enforcement of claims that a third party has illegally obtained and is using trade secrets is expensive, time consuming and uncertain. In addition, non-U.S. courts are sometimes less willing than U.S. courts to protect trade secrets. If our competitors independently develop equivalent knowledge, methods and know-how, we would not be able to assert our trade secrets against them and our business could be harmed.
34
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on all of our product candidates and products, when and if we have any, in every jurisdiction would be prohibitively expensive. Competitors may use our technologies in jurisdictions where we or our licensors have not obtained patent protection to develop their own products. These products may compete with our products, when and if we have any, and may not be covered by any of our or our licensors’ patent claims or other intellectual property rights.
The laws of some non-U.S. countries do not protect intellectual property rights to the same extent as the laws of the United States, and many companies have encountered significant problems in protecting and defending such rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property protection, particularly those relating to biotechnology and/or pharmaceuticals, which could make it difficult for us to stop the infringement of our patents. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial cost and divert our efforts and attention from other aspects of our business.
We may become involved in disputes with past or potential future collaborators over intellectual property ownership, and publications by our research collaborators and scientific advisors could impair our ability to obtain patent protection or protect our proprietary information, which, in either case, could have a significant effect on our business.
Inventions discovered under research, material transfer or other such collaborative agreements may become jointly owned by us and the other party to such agreements in some cases and the exclusive property of either party in other cases. Under some circumstances, it may be difficult to determine who owns a particular invention, or whether it is jointly owned, and disputes could arise regarding ownership of those inventions. These disputes could be costly and time consuming and an unfavorable outcome could have a significant adverse effect on our business if we were not able to protect or license rights to these inventions. In addition, our research collaborators and scientific advisors generally have contractual rights to publish our data and other proprietary information, subject to our prior review. Publications by our research collaborators and scientific advisors containing such information, either with our permission or in contravention of the terms of their agreements with us, may impair our ability to obtain patent protection or protect our proprietary information, which could significantly harm our business.
The intellectual property protection for our product candidates depends on third parties.
With respect to custirsen, apatorsen and OGX-225, we have exclusively licensed from UBC certain issued patents and pending patent applications covering the respective antisense sequences underlying these product candidates and their commercialization and use, and we have licensed from Ionis certain issued patents and pending patent applications directed to product compositions and chemical modifications used in product candidates for commercialization, use and the manufacturing thereof, as well as some alternative antisense sequences. We have also received a sublicense from Ionis under certain third-party patent portfolios directed to such modifications.
The patents and pending patent applications underlying our licenses do not cover all potential product candidates, modifications and uses. In the case of patents and patent applications licensed from Ionis, we do not have and have not had any control over the filing, prosecution or enforcement of these patents or patent applications. We cannot be certain that such prosecution efforts have been or will be conducted in compliance with applicable laws and regulations or will result in valid and enforceable patents. We also cannot be assured that our licensors or their respective licensing partners will agree to enforce any such patent rights at our request or devote sufficient efforts to attain a desirable result. Any failure by our licensors or any of their respective licensing partners to properly protect the intellectual property rights relating to our product candidates could have a material adverse effect on our financial condition and results of operation.
If we breach any of the agreements under which we license rights to our product candidates or technology from third parties, we could lose license rights that are important to our business. Certain of our license agreements may not provide an adequate remedy for a breach by the licensor.
We license the development and commercialization rights for most of our product candidates, including custirsen, apatorsen and OGX-225, and we expect to enter into similar licenses in the future. Under such licenses, we are subject to various obligations such as sublicensing, royalty and milestone payments, annual maintenance fees, limits on sublicensing, insurance obligations and the obligation to use commercially reasonable best efforts to develop and exploit the licensed technology. If we fail to comply with any of these obligations or otherwise breach these agreements, our licensors may have the right to terminate the license in whole or in part or to terminate the exclusive nature of the license. We may also become involved in disputes with licensors regarding the meaning of certain terms in the license agreements, including terms related to royalty and milestone payments, which may result in costly and time consuming litigation. Loss of any of these licenses or the exclusivity rights provided by the licenses could harm our financial condition and results of operations. In addition, certain of our license agreements with UBC eliminate our ability to obtain money damages in respect of certain claims against UBC.
35
If we are unable to successfully defend or settle our pending litigation with Ionis, we may be required to make a significant payment to Ionis and may lose certain development and commercialization rights related to our product candidates.
During 2015, we received communications from Ionis requesting payment of 30% of the $23.2 million paid by Teva under the Termination Agreement, as well as 30% of any amounts paid by Teva upon release of the $3.0 million holdback amount. In January 2016, Ionis filed a lawsuit and claimed that OncoGenex Technologies is in breach of the license agreement with Ionis for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva in connection with the termination of the Collaboration Agreement. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the license agreement. We do not, however, believe that any payments are due to Ionis. Under the Ionis license agreement, no payment is due to Ionis on any consideration that we receive for the reimbursement for research and development activities. The amounts paid or payable by Teva under the Termination Agreement constitute an advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, and therefore, no payments are owed to Ionis.
Litigation is costly and time consuming, and may result in a diversion of management’s attention and resources. If this litigation does not result in a successful outcome or we are otherwise unable to settle the dispute on acceptable terms, we may be required to pay Ionis a significant portion of the amounts that were paid by Teva, which may require us to revise our operating budget and clinical development plans, and delay or suspend clinical development. Ionis may also attempt to terminate the license agreement, which could result in our loss of certain development and commercialization rights relating to our product candidates and harm our ability to advance our product candidates.
The patent protection for our product candidates or products may expire before we are able to maximize their commercial value, which may subject us to increased competition and reduce or eliminate our opportunity to generate product revenue.
The patents for our product candidates have varying expiration dates and, when these patents expire, we may be subject to increased competition and we may not be able to recover our development costs. For example, certain of the U.S. patents directed to custirsen and its use that have been licensed from UBC are scheduled to expire in 2020 and 2021. In some of the larger economic territories, such as the United States and Europe, patent term extension/restoration may be available to compensate for time taken during aspects of the product candidate’s regulatory review. We cannot, however, be certain that an extension will be granted or, if granted, what the applicable time period or the scope of patent protection afforded during any extended period will be. In addition, even though some regulatory agencies may provide some other exclusivity for a product candidate under its own laws and regulations, we may not be able to qualify the product candidate or obtain the exclusive time period.
If we are unable to obtain patent term extension/restoration or some other exclusivity, we could be subject to increased competition and our opportunity to establish or maintain product revenue could be substantially reduced or eliminated. Furthermore, we may not have sufficient time to recover our development costs prior to the expiration of our U.S. and non-U.S. patents.
We may incur substantial costs as a result of litigation or other proceedings relating to patent and other intellectual property rights and we may be unable to protect our rights to, or use of, our technology.
If we choose to go to court to stop someone else from using the inventions claimed in our patents or our licensed patents, that individual or company has the right to ask the court to rule that these patents are invalid and/or should not be enforced against that third party. These lawsuits are expensive and would consume time and other resources even if we were successful in stopping the infringement of these patents. In addition, there is a risk that the court will decide that these patents are invalid or unenforceable and that we do not have the right to stop the other party from using the inventions. The U.S. Supreme Court has revised certain tests regarding granting patents and assessing the validity of patents to make it more difficult to obtain patents. Some of our issued patents may be subject to challenge and subsequent invalidation under the revised criteria. There is also the risk that, even if the validity or unenforceability of these patents is upheld, the court will narrow the scope of our claim or will refuse to stop the other party on the grounds that such other party’s activities do not infringe our rights.
If we wish to use the technology or compound claimed in issued and unexpired patents owned by others, we will need to obtain a license from the owner, enter into litigation to challenge the validity or enforceability of the patents or incur the risk of litigation in the event that the owner asserts that we infringed its patents. The failure to obtain a license to technology or the failure to challenge an issued patent that we may require to discover, develop or commercialize our product candidates may have a material adverse effect on us.
36
If a third party asserts that we infringed its patents or other proprietary rights, we could face a number of risks that could seriously harm our results of operations, financial condition and competitive position, including:
|
|
· |
patent infringement and other intellectual property claims, which would be costly and time consuming to defend, whether or not the claims have merit, and which could delay the regulatory approval process and divert management’s attention from our business; |
|
|
· |
substantial damages for past infringement, which we may have to pay if a court determines that our product candidates or technologies infringe a competitor’s patent or other proprietary rights; |
|
|
· |
a court prohibiting us from selling or licensing our technologies or future drugs unless the third party licenses its patents or other proprietary rights to us on commercially reasonable terms, which it is not required to do; and |
|
|
· |
if a license is available from a third party, we may have to pay substantial royalties or lump-sum payments or grant cross licenses to our patents or other proprietary rights to obtain that license. |
The biotechnology industry has produced a proliferation of patents, and it is not always clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform. If we are sued for patent infringement, we would need to demonstrate that our product candidates or methods of use either do not infringe the patent claims of the relevant patent, and/or that the patent claims are invalid, and/or that the patent is unenforceable and we may not be able to do this. Proving invalidity, in particular, is difficult since it requires a showing of clear and convincing evidence to overcome the presumption of validity enjoyed by issued patents.
U.S. patent laws as well as the laws of some foreign jurisdictions provide for provisional rights in published patent applications beginning on the date of publication, including the right to obtain reasonable royalties, if a patent subsequently issues and certain other conditions are met.
Because some patent applications in the United States may be maintained in secrecy until the patents are issued, because patent applications in the United States and many foreign jurisdictions are typically not published until 18 months after filing and because publications in the scientific literature often lag behind actual discoveries, we cannot be certain that others have not filed patent applications for technology covered by our licensors’ issued patents or our pending applications or our licensors’ pending applications, or that we or our licensors were the first to invent the technology.
Patent applications filed by third parties that cover technology similar to ours may have priority over our or our licensors’ patent applications and could further require us to obtain rights to issued patents covering such technologies. If another party files a U.S. patent application on an invention similar to ours, we may elect to participate in or be drawn into an interference proceeding declared by the U.S. Patent and Trademark Office to determine priority of invention in the United States. The costs of these proceedings could be substantial, and it is possible that such efforts would be unsuccessful, resulting in a loss of our U.S. patent position with respect to such inventions. Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources. In addition, any uncertainties resulting from the initiation and continuation of any litigation could have a material adverse effect on our ability to raise the funds necessary to continue our operations. We cannot predict whether third parties will assert these claims against us or against the licensors of technology licensed to us, or whether those claims will harm our business. If we are forced to defend against these claims, whether they are with or without any merit and whether they are resolved in favor of or against us or our licensors, we may face costly litigation and diversion of management’s attention and resources. As a result of these disputes, we may have to develop costly non-infringing technology, or enter into licensing agreements. These agreements, if necessary, may be unavailable on terms acceptable to us, if at all, which could seriously harm our business or financial condition.
We may be subject to damages resulting from claims that we, or our employees or consultants, have wrongfully used or disclosed alleged trade secrets of third parties.
Many of our employees were previously employed, and certain of our consultants are currently employed, at universities or biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although we have not received any claim to date, we may be subject to claims that these employees or consultants or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of these current or former employers. Litigation may be necessary to defend against these claims. If we fail in defending such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. We may be subject to claims that employees of our partners or licensors of technology licensed by us have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. We may become involved in litigation to defend against these claims. If we fail in defending such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel.
37
Risks Related to our Common Stock
The price for our common stock is volatile.
The market prices for our common stock and that of emerging life science companies generally have historically been highly volatile. For example, after the announcement of data from recent custirsen and apatorsen clinical trials, we experienced a significant decreases in our stock price. Future announcements concerning us, the results of our clinical trials or our competitors may also have a significant effect on the market price of our common stock. The stock markets also experience significant price and volume fluctuation unrelated to the operating performance of particular companies. These market fluctuations may also adversely affect the market price of our common stock.
An increase in the market price of our common stock, which is uncertain and unpredictable, may be the sole source of gain from an investment in our common stock. An investment in our common stock may not be appropriate for investors who require dividend income. We have never declared or paid cash dividends on our capital stock and do not anticipate paying any cash dividends on our capital stock in the foreseeable future. We currently intend to retain all available funds and any future earnings to fund the development and growth of our business. As a result, capital appreciation, if any, of our common stock will be the sole source of gain for stockholders for the foreseeable future. Accordingly, an investment in our common stock may not be appropriate for investors who require dividend income or investors who are not prepared to bear a significant risk of losses from such an investment.
The price of our common stock does not meet the requirements for continued listing on The NASDAQ Capital Market. If we fail to regain compliance with the minimum listing requirements, our common stock will be subject to delisting. Our ability to publicly or privately sell equity securities and the liquidity of our common stock could be adversely affected if our common stock is delisted.
The continued listing standards of The NASDAQ Capital Market require, among other things, that the minimum bid price of a listed company’s stock be at or above $1.00. If the minimum bid price is below $1.00 for a period of more than 30 consecutive trading days, the listed company will fail to be in compliance with The NASDAQ Capital Market’s listing rules and, if it does not regain compliance within the grace period, will be subject to delisting. As previously reported, on February 25, 2016, we received a notice from the NASDAQ Listing Qualifications Department notifying us that for 30 consecutive trading days, the bid price of our common stock had closed below the minimum $1.00 per share requirement. In accordance with The NASDAQ Capital Market’s listing rules, we were afforded 180 calendar days, or until August 23, 2016, to regain compliance with the bid price requirement. In order to regain compliance, the bid price of our common stock must close at a price of at least $1.00 per share for a minimum of 10 consecutive trading days. If we fail to regain compliance, our common stock will be subject to delisting. Delisting from The NASDAQ Capital Market could adversely affect our ability to raise additional financing through the public or private sale of equity securities, would significantly affect the ability of investors to trade our securities and would negatively affect the value and liquidity of our common stock. Delisting could also have other negative results, including the potential loss of confidence by employees, the loss of institutional investor interest and fewer business development opportunities
We are at risk of securities class action litigation.
In the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities, including in circumstances where such declines occur in close proximity to the announcement of clinical trial results. This risk is especially relevant for us because our stock price and those of other biotechnology and biopharmaceutical companies have experienced significant stock price volatility in recent years. If we face such litigation, it could result in substantial costs and a diversion of management’s attention and resources, which could harm our business.
If we raise additional capital, the terms of the financing transactions may cause dilution to existing stockholders or contain terms that are not favorable to us.
To date, our sources of cash have been limited primarily to proceeds from the private or public placement of our securities and reimbursement for custirsen-related development expenses from our prior strategic collaboration with Teva, which terminated in April 2015. In the future, we may seek to raise additional financing through private placements or public offerings of our equity or debt securities. We cannot be certain that additional funding will be available on acceptable terms, if at all. To the extent that we raise additional financing by issuing equity securities, we may do so at a price per share that represents a discount to the then-current per share trading price of our common stock and our stockholders may experience significant dilution. Any debt financing, if available, may involve restrictive covenants, such as limitations on our ability to incur additional indebtedness, limitations on our ability to acquire or license intellectual property rights and other operating restrictions that could adversely affect our ability to conduct our business.
38
Anti-takeover provisions in our stockholder rights plan, our charter documents and under Delaware law could make a third-party acquisition of us difficult.
We have a stockholder rights plan that may have the effect of discouraging unsolicited takeover proposals. Specifically, the rights issued under the stockholder rights plan could cause significant dilution to a person or group that attempts to acquire us on terms not approved in advance by our Board. In addition, our certificate of incorporation and bylaws contain provisions that may discourage unsolicited takeover proposals that stockholders may consider to be in their best interests. These provisions include the ability of our Board to designate the terms of and issue new series of preferred stock and the ability of our Board to amend our bylaws without stockholder approval. In addition, as a Delaware corporation, we are subject to Section 203 of the Delaware General Corporation Law, which generally prohibits a Delaware corporation from engaging in any business combination with any interested stockholder for a period of three years following the date that the stockholder became an interested stockholder, unless certain specific requirements are met as set forth in Section 203. Collectively, these provisions could make a third-party acquisition of us difficult or could discourage transactions that otherwise could involve payment of a premium over prevailing market prices for our common stock.
Risks Related to Our Industry
There is a high risk that our drug development activities will not result in commercial products.
Our product candidates are in various stages of development and are prone to the risks of failure inherent in drug development. We will need to complete significant additional clinical trials before we can demonstrate that our product candidates are safe and effective to the satisfaction of regulatory agencies. Clinical trials are expensive and uncertain processes that take years to complete. Failure can occur at any stage of the process, and successful early clinical trials do not ensure that later clinical trials will be successful. Product candidates in later-stage clinical trials may fail to show desired efficacy and safety traits despite having progressed through initial clinical trials. For example, in April 2014, we announced that top-line survival results indicated that the addition of custirsen to standard first-line docetaxel/prednisone therapy did not meet the primary endpoint of a statistically significant improvement in overall survival in men with metastatic CRPC, compared to docetaxel/prednisone alone. Additionally, in January 2016, we announced that data from the phase 2 Spruce trial evaluating the combination of apatorsen with carboplatin and pemetrexed in patients with untreated metastatic NSCLC did not reach the statistical significance required to demonstrate a PFS benefit. A number of companies in the pharmaceutical industry have suffered significant setbacks in advanced clinical trials, even after obtaining promising results in earlier clinical trials. In addition, a clinical trial may prove successful with respect to a secondary objective, but fail to demonstrate clinically significant benefits with respect to a primary objective. Failure to satisfy a primary objective in a phase 3 clinical trial (registration trial) would generally mean that a product candidate would not receive regulatory approval.
The regulatory approval process is expensive, time consuming and uncertain and may prevent us from obtaining approvals for the commercialization of some or all of our product candidates.
The research, testing, manufacturing, labeling, approval, selling, marketing and distribution of drug products are subject to extensive regulation by regulatory agencies, which regulations differ from country to country. We are not permitted to market our product candidates in the United States until we receive approval of an application for market approval from regulatory agencies. We have not submitted an application for or received marketing approval for any of our product candidates. Obtaining approval of an application for market approval can be a lengthy, expensive and uncertain process. In addition, failure to comply with regulatory agencies’ requirements may, either before or after product approval, if any, subject us to administrative or judicially imposed sanctions, including:
|
|
· |
restrictions on the products, manufacturers or manufacturing process; |
|
|
· |
warning letters; |
|
|
· |
civil and criminal penalties; |
|
|
· |
injunctions; |
|
|
· |
suspension or withdrawal of regulatory approvals; |
|
|
· |
product seizures, detentions or import bans; |
|
|
· |
voluntary or mandatory product recalls and publicity requirements; |
|
|
· |
total or partial suspension of production; |
|
|
· |
imposition of restrictions on operations, including costly new manufacturing requirements; and |
|
|
· |
refusal to approve pending applications for market approval or supplements to approved applications for market approval. |
Regulatory approval of an application for market approval or application for market approval supplement is not guaranteed, and the approval process is expensive and may take several years. Regulatory agencies also has substantial discretion in the drug approval
39
process. Even though we have received support for our protocol amendment to the AFFINITY trial, this does not guarantee that regulatory agencies will be supportive of an application for market approval. Despite the time and expense exerted, failure can occur at any stage, and we could encounter problems that could cause us to abandon clinical trials or to repeat or perform additional preclinical studies and clinical trials. The number of preclinical studies and clinical trials that will be required for regulatory agencies’ approval varies depending on the drug candidate, the disease or condition that the drug candidate is designed to address, and the regulations applicable to any particular drug candidate. Regulatory agencies can delay, limit or deny approval of a drug candidate for many reasons, including:
|
|
· |
a drug candidate may not be deemed safe or effective; |
|
|
· |
regulatory agencies may not find the data from preclinical studies and/or clinical trials sufficient; |
|
|
· |
regulatory agencies might not approve our third-party manufacturer’s processes or facilities; |
|
|
· |
regulatory agencies may change its approval policies or adopt new regulations; and |
|
|
· |
third-party products may enter the market and change approval requirements. |
Even if we obtain regulatory approvals for our product candidates, the terms of approvals and ongoing regulation of our product candidates may limit how we manufacture and market our product candidates, which could materially affect our ability to generate revenue.
If any of our product candidates are approved, the approved product and its manufacturer will be subject to continual review. Any regulatory approval that we receive for a product candidate is likely to be subject to limitations on the indicated uses for which the end product may be marketed, or include requirements for potentially costly post-approval follow-up clinical trials. In addition, if regulatory agencies approve any of our product candidates, the labeling, packaging, adverse event reporting, storage, advertising and promotion for the end product will be subject to extensive regulatory requirements. We and the manufacturers of our products, when and if we have any, will also be required to comply with cGMP regulations, which include requirements relating to quality control and quality assurance, as well as the corresponding maintenance of records and documentation. Further, regulatory agencies must approve these manufacturing facilities before they can be used to manufacture our products, when and if we have any, and these facilities are subject to ongoing regulatory inspection. If we fail to comply with the regulatory requirements of regulatory agencies, or if previously unknown problems with our products, when and if we have any, manufacturers or manufacturing processes are discovered, we could be subject to administrative or judicially imposed sanctions, including:
|
|
· |
restrictions on the products, manufacturers or manufacturing process; |
|
|
· |
warning letters; |
|
|
· |
civil or criminal penalties or fines; |
|
|
· |
injunctions; |
|
|
· |
product seizures, detentions or import bans; |
|
|
· |
voluntary or mandatory product recalls and publicity requirements; |
|
|
· |
suspension or withdrawal of regulatory approvals; |
|
|
· |
total or partial suspension of production; |
|
|
· |
imposition of restrictions on operations, including costly new manufacturing requirements; and |
|
|
· |
refusal to approve pending applications for market approval or supplements to approved applications for market approval. |
In addition, regulatory agencies may change their policies and additional regulations may be enacted that could prevent or delay regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the United States, Canada or abroad. If we are not able to maintain regulatory compliance, we would likely not be permitted to market our future product candidates and we may not achieve or sustain profitability.
If government and third-party payors fail to provide coverage and adequate reimbursement rates for our product candidates, our revenue and potential for profitability will be reduced.
In the United States and elsewhere, our product revenue will depend principally on the reimbursement rates established by third-party payors, including government health administration authorities, managed-care providers, public health insurers, private health insurers and other organizations. These third-party payors are increasingly challenging the price, and examining the cost-effectiveness, of medical products and services. In addition, significant uncertainty exists as to the reimbursement status, if any, of newly approved
40
drugs, pharmaceutical products or product indications. We may need to conduct post-marketing clinical trials in order to demonstrate the cost-effectiveness of our products, if any. Such clinical trials may require us to commit a significant amount of management time and financial and other resources. If reimbursement of such product is unavailable or limited in scope or amount or if pricing is set at unsatisfactory levels, our revenue could be reduced.
In some countries other than the United States, particularly the countries of the European Union and Canada, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, obtaining pricing approval from governmental authorities can take six to 12 months or longer after the receipt of regulatory marketing approval of a product for an indication. To obtain reimbursement or pricing approval in some countries, we may be required to conduct a clinical trial that compares the cost-effectiveness of one of our product candidates to other available therapies. If reimbursement of such product candidate is unavailable or limited in scope or amount or if pricing is set at unsatisfactory levels, our revenue could be reduced.
Domestic and foreign governments continue to propose and pass legislation designed to reduce the cost of healthcare, including drugs. In the United States, there have been, and we expect that there will continue to be, federal and state proposals to implement similar governmental control. In addition, increasing emphasis on managed care in the United States will continue to put pressure on the pricing of pharmaceutical products. For example, in March 2010, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, or collectively, PPACA, became law in the United States. PPACA substantially changes the way healthcare is financed by both governmental and private insurers and significantly affects the pharmaceutical industry.
We anticipate that the PPACA, as well as other healthcare reform measures that may be adopted in the future, may result in more rigorous coverage criteria and downward pressure on the price for any approved product, and could seriously harm our prospects. In addition, the Medicare and Medicaid program and state healthcare laws and regulations may also be modified to change the scope of covered products and/or reimbursement methodology. Cost control initiatives could decrease the established reimbursement rates that we receive for any products in the future, which would limit our revenue and profitability. Legislation and regulations affecting the pricing of pharmaceutical products, including custirsen, or apatorsen may change at any time, which could further limit or eliminate reimbursement rates for custirsen, apatorsen or other product candidates.
Failure to obtain regulatory approval outside of the United States and Canada would prevent us from marketing our product candidates abroad.
We intend to market certain of our existing and future product candidates outside of the United States and Canada. In order to market our existing and future product candidates in the European Union and many other non-North American markets, we must obtain separate regulatory approvals. We have had limited interactions with non-North American regulatory authorities. Approval procedures vary among countries and can involve additional testing, and the time required to obtain approval may differ from that required to obtain FDA approval. Approval by the FDA or other regulatory authorities does not ensure approval by regulatory authorities in other countries, and approval by one or more non-North American regulatory authorities does not ensure approval by regulatory authorities in other countries or by the FDA. The non-North American regulatory approval process may include all of the risks associated with obtaining FDA approval. We may not obtain non-North American regulatory approvals on a timely basis, if at all. We may not be able to file for non-North American regulatory approvals and may not receive necessary approvals to commercialize our existing and future product candidates in any market.
None.
We have business offices located in Bothell, Washington and Vancouver, British Columbia.
Our lease agreement for office space in Bothell, Washington commenced on February 15, 2015 and has a three-year term with one three-year renewal option. Pursuant to this lease, we rent approximately 13,771 square feet of office space. The annual rent is approximately $0.3 million.
We lease approximately 4,857 square feet in Vancouver, British Columbia, currently at an annual rent of approximately CND $0.1 million, which lease expires in September 2016.
We believe that the facilities we currently lease are sufficient for our anticipated near-term needs.
41
On January 5, 2016, Ionis Pharmaceuticals, Inc. (formerly known as Isis Pharmaceuticals, Inc.) filed a lawsuit against our subsidiary OncoGenex Technologies, Inc. in the United States District Court for the Southern District of California. Ionis claims that OncoGenex Technologies is in breach of an Amended and Restated License Agreement between Ionis and OncoGenex Technologies dated July 2, 2008, as amended, or License Agreement. Under the License Agreement, Ionis is entitled to a share of certain forms of non-royalty revenue received by OncoGenex Technologies, but is not entitled to a share of revenue received by OncoGenex Technologies for the reimbursement of research and development activities. In April 2015, we terminated a collaboration agreement with Teva Pharmaceuticals Industries Ltd. In connection with that termination, Teva paid us $23.2 million as an advance reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin. In the lawsuit, Ionis claims that OncoGenex Technologies is in breach of the License Agreement for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the License Agreement. On March 4, 2016, OncoGenex Technologies filed a motion to dismiss the lawsuit in the United States District Court for the Southern District of California.
We intend to vigorously defend this matter and, based on our preliminary review, we believe we have valid defenses. However, litigation is inherently uncertain, and any judgment or injunctive relief entered against us or any adverse settlement could materially and adversely impact our business, financial condition, operating results and prospects. Because we are in the early stages of this matter, we are unable to estimate a reasonably possible range of loss, if any, that may result from this matter. In addition, litigation can involve significant management time and attention, and the cost of litigation can be expensive, regardless of outcome.
Not applicable.
42
|
MARKET FOR THE REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Our common stock first began trading on the Nasdaq National Market under the symbol “SNUS” on October 12, 1995. Following the completion of the Arrangement discussed elsewhere in this Annual Report on Form 10-K, our common stock commenced trading on the Nasdaq Capital Market under the stock symbol “OGXI”, effective August 21, 2008.
No cash dividends have been paid on our common stock, and we do not anticipate paying any cash dividends in the foreseeable future. As of February 15, 2016, there were approximately 87 stockholders of record and there were approximately 9,436 beneficial stockholders of our common stock. The high and low sales prices of our common stock as reported by the NASDAQ Capital Market for the periods indicated are as follows:
|
OncoGenex Pharmaceuticals, Inc. |
|
HIGH |
|
|
LOW |
|
||
|
|
|
|
|
|
|
|
|
|
|
YEAR ENDED DECEMBER 31, 2014: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First quarter |
|
$ |
14.25 |
|
|
$ |
8.30 |
|
|
Second quarter |
|
|
12.09 |
|
|
|
3.26 |
|
|
Third quarter |
|
|
3.84 |
|
|
|
2.63 |
|
|
Fourth quarter |
|
|
2.67 |
|
|
|
1.98 |
|
|
|
|
|
|
|
|
|
|
|
|
YEAR ENDED DECEMBER 31, 2015: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First quarter |
|
$ |
2.78 |
|
|
$ |
1.92 |
|
|
Second quarter |
|
|
3.10 |
|
|
|
1.74 |
|
|
Third quarter |
|
|
4.10 |
|
|
|
1.38 |
|
|
Fourth quarter |
|
|
2.80 |
|
|
|
1.11 |
|
The information required by this item regarding equity compensation plan information is set forth in Part III, Item 12 of this Annual Report on Form 10-K. No purchases of equity securities during the year ended December 31, 2015 were made by us or on our behalf and we did not sell any unregistered securities during such year.
43
Stock Performance Graph
The following performance graph shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or incorporated by reference into any of our filings under the Securities Act or the Exchange Act, except as expressly set forth by specific reference in such filings. The graph compares the cumulative five-year total return provided to stockholders on our common stock relative to the cumulative total returns of the NASDAQ Composite Index and the NASDAQ Pharmaceutical Index. An investment of $100 (with reinvestment of all dividends into additional shares of the same class of equity securities at the frequency with which dividends are paid on such securities during the applicable year) is assumed to have been made in our common stock and in each of the indexes on December 31, 2010 and its relative performance is tracked through December 31, 2015.
The stock price performance included in this graph is not necessarily indicative of future stock price performance.
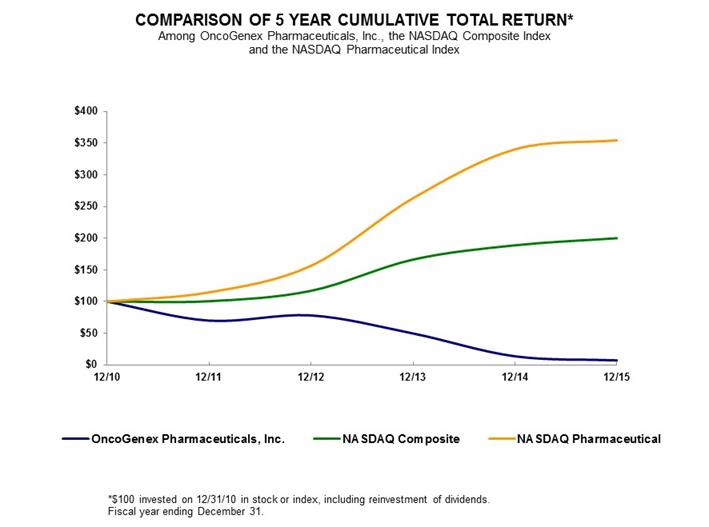
|
|
|
12/31/10 |
|
|
12/31/11 |
|
|
12/31/12 |
|
|
12/31/13 |
|
|
12/31/14 |
|
|
12/31/15 |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OncoGenex Pharmaceuticals, Inc. |
|
|
100.00 |
|
|
|
69.92 |
|
|
|
78.14 |
|
|
|
49.67 |
|
|
|
13.64 |
|
|
|
7.21 |
|
|
NASDAQ Composite |
|
|
100.00 |
|
|
|
100.53 |
|
|
|
116.92 |
|
|
|
166.19 |
|
|
|
188.78 |
|
|
|
199.95 |
|
|
NASDAQ Pharmaceutical |
|
|
100.00 |
|
|
|
114.48 |
|
|
|
156.39 |
|
|
|
263.04 |
|
|
|
340.07 |
|
|
|
354.40 |
|
The data set forth below should be read in conjunction with Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and the Consolidated Financial Statements and Notes thereto appearing at Item 8 of this Annual Report on Form 10-K. The selected consolidated statements of loss data for the years ended December 31, 2015, 2014 and 2013 and consolidated balance sheet data as of December 31, 2015 and 2014 set forth below have been derived from our audited consolidated financial statements included elsewhere in this Annual Report on Form 10-K. The selected statements of loss data for the year ended December 31, 2012 and 2011 and the balance sheet data as of December 31, 2013, 2012 and 2011 set forth below have been derived from the audited consolidated financial statements for such years not included in this Annual Report on Form 10-K.
44
The historical results presented are not necessarily indicative of future results.
|
|
|
December 31, |
|
|||||||||||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|
2012 |
|
|
2011 |
|
|||||
|
|
|
(in thousands except share and per share amounts) |
|
|||||||||||||||||
|
Statements of Loss Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Collaboration revenue |
|
$ |
18,160 |
|
|
$ |
27,116 |
|
|
$ |
29,882 |
|
|
$ |
20,095 |
|
|
$ |
5,496 |
|
|
Total expenses |
|
$ |
36,913 |
|
|
$ |
53,332 |
|
|
$ |
65,209 |
|
|
$ |
46,082 |
|
|
$ |
27,783 |
|
|
Net loss |
|
$ |
(16,801 |
) |
|
$ |
(26,240 |
) |
|
$ |
(31,849 |
) |
|
$ |
(21,098 |
) |
|
$ |
(14,673 |
) |
|
Basic and diluted loss per common share |
|
$ |
(0.64 |
) |
|
$ |
(1.45 |
) |
|
$ |
(2.17 |
) |
|
$ |
(1.56 |
) |
|
$ |
(1.51 |
) |
|
Shares used in calculation of net loss per share |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Basic and diluted |
|
|
26,147,344 |
|
|
|
18,098,799 |
|
|
|
14,683,389 |
|
|
|
13,522,723 |
|
|
|
9,729,340 |
|
|
|
|
December 31, |
|
|||||||||||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|
2012 |
|
|
2011 |
|
|||||
|
|
|
(in thousands) |
|
|||||||||||||||||
|
Balance Sheet Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash, cash equivalents and short-term investments |
|
$ |
55,186 |
|
|
$ |
47,057 |
|
|
$ |
39,222 |
|
|
$ |
75,383 |
|
|
$ |
64,927 |
|
|
Total assets |
|
$ |
58,209 |
|
|
$ |
56,291 |
|
|
$ |
55,689 |
|
|
$ |
82,016 |
|
|
$ |
68,015 |
|
|
Current liabilities |
|
$ |
20,664 |
|
|
$ |
22,218 |
|
|
$ |
14,934 |
|
|
$ |
11,556 |
|
|
$ |
30,786 |
|
|
Total liabilities |
|
$ |
20,769 |
|
|
$ |
22,232 |
|
|
$ |
18,478 |
|
|
$ |
15,809 |
|
|
$ |
37,125 |
|
|
Additional paid-in capital |
|
$ |
211,590 |
|
|
$ |
191,373 |
|
|
$ |
168,242 |
|
|
$ |
165,395 |
|
|
$ |
108,986 |
|
|
Accumulated deficit |
|
$ |
(176,811 |
) |
|
$ |
(159,958 |
) |
|
$ |
(133,689 |
) |
|
$ |
(101,840 |
) |
|
$ |
(80,742 |
) |
|
Stockholders’ equity |
|
$ |
37,440 |
|
|
$ |
34,059 |
|
|
$ |
37,211 |
|
|
$ |
66,207 |
|
|
$ |
30,890 |
|
Forward-Looking Statements
This Annual Report on Form 10-K contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. These forward-looking statements involve a number of risks and uncertainties. We caution readers that any forward-looking statement is not a guarantee of future performance and that actual results could differ materially from those contained in the forward-looking statement. These statements are based on current expectations of future events. Such statements include, but are not limited to, statements about future financial and operating results, plans, objectives, expectations and intentions, costs and expenses, interest rates, outcome of contingencies, financial condition, results of operations, liquidity, business strategies, cost savings, objectives of management and other statements that are not historical facts. You can find many of these statements by looking for words like “believes,” “expects,” “anticipates,” “estimates,” “may,” “should,” “will,” “could,” “plan,” “intend,” or similar expressions in this Annual Report on Form 10-K or in documents incorporated by reference into this Annual Report on Form 10-K . We intend that such forward-looking statements be subject to the safe harbors created thereby. Examples of these forward-looking statements include, but are not limited to:
|
|
· |
progress and preliminary and future results of clinical trial; |
|
|
· |
anticipated regulatory filings, requirements and future clinical trials; |
|
|
· |
timing and amount of future contractual payments, product revenue and operating expenses; |
|
|
· |
market acceptance of our products and the estimated potential size of these markets; and |
|
|
· |
our anticipated future capital requirements and the terms of any capital financing agreements. |
These forward-looking statements are based on the current beliefs and expectations of our management and are subject to significant risks and uncertainties. If underlying assumptions prove inaccurate or unknown risks or uncertainties materialize, actual results may differ materially from current expectations and projections. Factors that might cause such a difference include those discussed in Item 1A “Risk Factors,” as well as those discussed elsewhere in the Annual Report on Form 10-K.
You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this Annual Report on Form 10-K or, in the case of documents referred to or incorporated by reference, the date of those documents.
45
All subsequent written or oral forward-looking statements attributable to us or any person acting on our behalf are expressly qualified in their entirety by the cautionary statements contained or referred to in this section. We do not undertake any obligation to release publicly any revisions to these forward-looking statements to reflect events or circumstances after the date of this Annual Report on Form 10-K or to reflect the occurrence of unanticipated events, except as may be required under applicable U.S. securities law. If we do update one or more forward-looking statements, no inference should be drawn that we will make additional updates with respect to those or other forward-looking statements.
Overview
We are an emerging leader in next generation cancer therapeutics. Our mission is to accelerate transformative therapies to improve the lives of people living with cancer and other serious diseases. We have developed a pipeline of late-stage product candidates that are designed to block the production of specific proteins that promote treatment resistance in cancer. We believe our therapies have the potential to redefine treatment outcomes in a variety of cancers. We have three product candidates in our pipeline: custirsen, apatorsen and OGX-225, each of which has a distinct mechanism of action and represents a unique opportunity for cancer drug development. Of the product candidates in our pipeline, custirsen and apatorsen are clinical-stage assets being evaluated in two phase 3 studies and four phase 2 studies, respectively.
Our product candidates -- custirsen, apatorsen and OGX-225 -- focus on mechanisms of treatment resistance in cancer patients and are designed to block the production of specific proteins that we believe promote treatment resistance and survival of tumor cells and are over-produced in response to a variety of cancer treatments. Our aim in targeting these particular proteins is to disable the tumor cell’s adaptive defenses, thereby rendering the tumor cells more susceptible to attack with a variety of cancer therapies. We believe this approach will increase survival time and improve the quality of life for cancer patients.
In February 2016, we committed to a plan to reduce operating expenses, which included a workforce reduction of 11 employees, representing approximately 27% of our employees prior to the reduction. We estimate we will incur approximately $0.4 million in cash expenditures as a result of the workforce reduction, substantially all of which will be severance costs. We expect cost savings associated with the reduction of employees and consultants, together with the elimination of certain planned expenditures not required for the completion of ongoing trials, will extend our cash runway into the third quarter of 2017. We plan to remain focused on executing clinical development plans in order to reach several near-term milestones for both the custirsen and apatorsen programs.
Product Candidate Custirsen
Three phase 3 custirsen clinical trials have been initiated:
|
|
· |
The SYNERGY Trial: The completed phase 3 clinical trial evaluated a survival benefit for custirsen in combination with first-line docetaxel treatment in patients with metastatic castrate resistant prostate cancer, or metastatic CRPC. Results of the SYNERGY trial were presented at the European Society for Medical Oncology (ESMO) 2014 Congress in September 2014. Final survival results indicated that the addition of custirsen to standard first-line docetaxel/prednisone therapy did not meet the primary endpoint of a statistically significant improvement in overall survival, or OS, in men with metastatic CRPC, compared to docetaxel/prednisone alone (median survival 23.4 months vs. 22.2 months, respectively; hazard ratio 0.93 and one-sided p value 0.207). The adverse events observed were similar to custirsen's known adverse event profile. Subsequent exploratory analyses showed improved overall survival for those men who received custirsen and who were at increased risk for poor outcomes. Those preliminary results showed a 27% lower rate of death for patients who were at increased risk for poor outcomes and received custirsen. Based on these findings, we have amended the AFFINITY trial as outlined below. |
|
|
· |
The AFFINITY Trial: The phase 3 clinical trial to evaluate a survival benefit for custirsen in combination with cabazitaxel treatment as second-line chemotherapy in patients with CRPC. AFFINITY was initiated in August 2012 and completed enrollment of approximately 630 patients in September 2014. In January 2015, an interim futility analysis was completed and per recommendation of an Independent Data Monitoring Committee, or IDMC, the trial continued as planned. |
Based on the exploratory findings from the SYNERGY trial, we sought advice from regulatory authorities to amend the AFFINITY trial to include these learnings and to adjust the statistical analysis plan accordingly. Both the FDA and European Medicines Agency, or EMA, were supportive of the proposed amendment to the AFFINITY protocol and statistical analysis plan. The following protocol amendment was submitted in all participating countries where the trial is being conducted:
|
|
o |
The inclusion of a co-primary survival objective for evaluating survival benefit in a subpopulation of men who were at increased risk for poor outcomes as well as for all men enrolled into the study, known as the intent-to-treat (ITT) population. |
46
|
|
o |
A revised statistical analysis plan including the hypothesized hazard ratio, or HR, for the subpopulation who are at an increased risk for poor outcomes specified to be 0.69 with the critical HR ≤ 0.778. The hypothesized HR for the ITT population, remains unchanged as 0.75 with the critical HR ≤ 0.820. |
|
|
o |
The revised statistical analysis plan included an interim analysis for the ITT population at the same time as the final analysis for the subpopulation. This interim analysis had both futility and early efficacy criteria defined for the ITT population. |
The co-primary survival analysis for the poor prognostic subpopulation and the interim analysis for the ITT population in the AFFINITY trial were completed in December 2015. The co-primary survival results for the subpopulation of men who had multiple poor prognostic risk factors revealed that the combination of custirsen and cabazitaxel did not meet the rigorous criteria required to demonstrate an improvement in overall survival (hypothesized hazard ratio < 0.69, one-sided p value < 0.015). Based on the interim analysis for the ITT population, the IDMC recommended that the trial continue as planned. Both the IDMC and we remain blinded to all analyses and final results are expected in the third quarter of 2016, depending on timing of the event-driven final ITT analysis.
|
|
· |
The ENSPIRIT Trial: The phase 3 clinical trial to evaluate a survival benefit for custirsen in combination with docetaxel treatment as second-line chemotherapy in patients with NSCLC. This trial was initiated in September 2012. |
The first interim futility analysis was completed in August 2014. A protocol amendment was submitted and approved by all regulatory agencies in participating countries, to amend the statistical design and analysis plan of the ENSPIRIT trial including the following:
|
|
o |
A revised statistical analysis plan including the hypothesized HR, to be 0.75 with the critical HR of ≤ 0.84, reducing the required sample size from 1,100 to 700 patients. This change maintained 90% power while assessing for a more clinically relevant survival benefit when adding custirsen to second-line docetaxel. |
|
|
o |
A revision to the final interim futility analysis with more rigorous criteria in order to continue the trial due to lack of futility. This was successfully completed in July 2015, and the trial continued as planned. |
|
|
o |
The inclusion of an additional objective to analyze survival outcome based on NSCLC histology as part of the other non-primary analyses. |
We believe these amendments, specifically the revised statistical thresholds, are more appropriately aligned to the interests of both treating clinicians and their patients. Based on current ENSPIRIT enrollment projections and the changes outlined in the protocol amendment, we believe final survival results could be available in the first half of 2017, depending on completion of enrollment and timing of the event-driven final analysis.
Custirsen has received Fast Track designation from the U.S. Food and Drug Administration, or FDA, for second-line treatment of metastatic CRPC when combined with cabazitaxel and prednisone and for the second-line treatment of advanced NSCLC when combined with docetaxel in patients with disease progression following treatment with a first-line, platinum-based chemotherapy doublet regimen.
We and collaborating investigators have completed one phase 3 clinical trial and five phase 2 clinical trials to evaluate the ability of custirsen to enhance the effects of therapy in prostate, non-small cell lung and breast cancers. Results have been presented for each of these trials. Refer to the discussions in Part I, Item 1 under the headings “Our Product Candidates—Custirsen— Current Custirsen Development Activities” and “Our Product Candidates—Custirsen —Summary of Results of Custirsen Clinical Trials” for further details.
Product Candidate Apatorsen
Apatorsen is our product candidate that is designed to inhibit production of Hsp27, a cell-survival protein expressed in many types of cancers including bladder, prostate, breast, pancreatic and non-small cell lung cancer. Hsp27 expression is stress-induced, including by many anti-cancer therapies. Overexpression of Hsp27 is thought to be an important factor leading to the development of treatment resistance and is associated with metastasis and negative clinical outcomes in patients with various tumor types.
A number of preclinical studies have shown that reducing Hsp27 production induces tumor cell death in prostate, non-small cell lung, bladder and pancreatic cancer cells. The studies also suggest that reducing Hsp27 production sensitizes prostate tumor cells to hormone ablation therapy. These preclinical studies have also shown that inhibiting the production of Hsp27 in human prostate, bladder, lung, breast, ovarian and pancreatic tumor cells sensitizes the cells to chemotherapy.
Hsp27 has been reported by others to function as an immunomodulatory protein by a number of mechanisms that include altering important membrane expressed proteins on monocytes and immature dendritic cells; this alteration results in tumor-associated immune cells that are not functional in identifying and killing cancer cells. The induction of anti-inflammatory cytokines by Hsp27 may also play a role in down-regulating lymphocyte activation leading to additional unresponsive immune cells.
47
In 2013, we initiated the ORCA (Ongoing Studies Evaluating Treatment Resistance in CAncer) program which encompasses clinical studies designed to evaluate whether inhibition of Hsp27 can lead to improved prognosis and treatment outcomes for cancer patients. Our goal is to advance cancer treatment by conducting clinical trials for apatorsen across multiple cancer indications including bladder, lung, pancreatic and prostate cancers. We are conducting parallel clinical trials to evaluate apatorsen in several cancer indications and treatment combinations to accelerate the development of apatorsen. As part of this strategy, we are supporting specific investigator-sponsored trials to allow assessment of a broader range of clinical indications for future OncoGenex-sponsored trials and possible market approval. The ORCA trials, with exception of the Pacific™ trial, are designed to provide information that will be useful for designing future phase 3 trials and may be used as supportive studies for registration, if applicable. Due to small sample sizes, data from these trials are not likely to result in statistically significant differences in either PFS or survival.
Six phase 2 apatorsen clinical trials have been initiated or completed under the ORCA program.

Completed Trials
|
|
· |
The Borealis-1™ Trial: Our completed company-sponsored Borealis-1™ phase 2 trial was a three-arm, randomized, placebo-controlled trial evaluating apatorsen in combination with a first-line standard of care chemotherapy regimen (gemcitabine and cisplatin) in the metastatic setting. Results from an exploratory analysis showed that metastatic bladder cancer patients with poor prognostic features (lower performance status, liver involvement, low hemoglobin and high alkaline phosphatase) benefited from the addition of 600mg apatorsen to first-line chemotherapy (OS HR = 0.72) compared to chemotherapy alone. Patients in the trial with a Karnofsky Performance Status (KPS) of 80% or less, a common indicator of poor prognosis, experienced a 50% reduction in risk of death with the addition of apatorsen therapy (OS HR = 0.50). These results were presented in an oral session on June 1, 2015 at ASCO and additional analyses were presented on September 28, 2015 at the European Cancer Congress, or ECC. |
|
|
· |
The Rainier™ Trial: Our completed investigator-sponsored Rainier™ phase 2 trial was a randomized, placebo-controlled trial evaluating apatorsen in combination with ABRAXANE® (paclitaxel protein-bound particles for injectable suspension) (albumin-bound) and gemcitabine compared to ABRAXANE and gemcitabine alone in patients with untreated metastatic pancreatic cancer. The addition of apatorsen to ABRAXANE and gemcitabine did not demonstrate an overall survival benefit in the study when compared to ABRAXANE and gemcitabine alone. A potential benefit was observed in a subgroup of patients with high baseline serum Hsp27 status (14% of total) when treated with apatorsen (PFS HR= 0.40; 95% CI 0.19-0.86 and survival HR= 0.57; 95% CI 0.26-1.25). Overall, higher baseline Hsp27 status correlated with worse survival outcome. The study was sponsored and conducted by Sarah Cannon Research Institute, or SCRI, and further results were presented at the Gastrointestinal, or GI, Cancers Symposium meeting in January 2016. The study investigators concluded that these promising results in pancreatic cancer patients with Hsp27 high status warrant further study of apatorsen in this population. OncoGenex does not intend to pursue additional trials in pancreatic cancer at this time. |
Ongoing Trials
|
|
· |
The Borealis-2™ Trial: The investigator-sponsored, randomized phase 2 trial evaluating apatorsen in combination with docetaxel treatment compared to docetaxel treatment alone in patients with advanced or metastatic bladder cancer who have disease progression following first-line platinum-based chemotherapy. Patients may also continue weekly apatorsen infusions as maintenance treatment until disease progression or unacceptable toxicity if they complete all 10 cycles of docetaxel, or are discontinued from docetaxel due to docetaxel toxicity. This trial was initiated in April 2013 and patient enrollment was completed in September 2015. The trial randomized approximately 200 patients and results are expected in the second half of 2016. |
|
|
· |
The Spruce™ Trial: The investigator-sponsored, randomized, placebo-controlled phase 2 trial evaluating apatorsen plus carboplatin and pemetrexed therapy compared to carboplatin and pemetrexed therapy in patients with previously untreated advanced non-squamous NSCLC. Patients continued weekly apatorsen or placebo infusions as maintenance treatment until disease progression if they completed a minimum of 3 cycles of chemotherapy treatment. The aim of the trial is to determine if adding apatorsen to carboplatin and pemetrexed therapy can extend PFS outcome. Additional analyses are expected to include tumor response rates, overall survival, safety, tolerability and the effect of therapy on Hsp27 levels. Patients who are at increased risk for poor outcomes will also be prospectively evaluated. This trial was initiated in August 2013 and patient enrollment was completed in February 2015. The trial randomized approximately 155 patients. Primary endpoint data for PFS was reported in January 2016 and did not reach the statistical significance required to |
48
|
|
demonstrate a benefit. A potential PFS benefit was observed in patients with high baseline serum Hsp27 status when treated with apatorsen. The study is ongoing and overall survival results are expected in the second half of 2016. |
|
|
· |
The Spruce-2™ Trial (formerly referred to as the Cedar Trial): The investigator-sponsored, randomized phase 2 trial evaluating apatorsen plus gemcitabine and carboplatin therapy or gemcitabine and carboplatin therapy alone in patients with previously untreated advanced squamous NSCLC. Patients also continue weekly apatorsen infusions as maintenance treatment after chemotherapy until disease progression. The aim of the trial is to determine if adding apatorsen to gemcitabine and carboplatin therapy can extend PFS outcome. Additional analyses will include tumor response rates, overall survival, safety, and health-related quality of life. Additional analyses are expected to determine the effect of therapy on Hsp27 levels, explore potential biomarkers that may help predict response to treatment and survival outcomes in patients who were at increased risk for poor outcomes. The trial was initiated in July 2014 and is enrolling patients. The trial is expected to randomize approximately 140 patients. |
|
|
· |
The Pacific™ Trial: The investigator-sponsored, randomized phase 2 trial evaluating apatorsen in men with CRPC who are experiencing a rising PSA while receiving Zytiga® (abiraterone acetate). The aim of the trial is to determine if adding apatorsen to Zytiga treatment can reverse or delay treatment resistance by evaluating the PFS rate at a milestone Day 60 assessment. Other secondary endpoints such as PSA and objective responses, time to disease progression, CTCs and Hsp27 levels are expected to be evaluated. The trial completed enrollment of 72 patients in March 2016. |
In addition to the Borealis-1 and Borealis-2 clinical trials in metastatic bladder cancer in the ORCA program, we are evaluating apatorsen for the potential treatment of NMIBC. We have completed a pre-IND meeting with FDA in preparation for a separate IND application to evaluate apatorsen for intravesical administration in combination with Bacillus Calmette-Guerin, or BCG, treatment in patients with NMIBC. FDA had no objection to the study population or classification of subpopulations in the proposed study design and deemed the proposed definitions of primary and secondary endpoints acceptable.
Refer to the discussion in Part I, Item 1 under the heading “Our Product Candidates—Apatorsen—Summary of Results of Apatorsen Clinical Trials” for further details.
Product Candidates OGX-225
OGX-225 is our product candidate designed to inhibit the production of Insulin Growth Factor Binding Proteins -2 and -5 (IGFBP-2, IGFBP-5), two proteins that when overexpressed affect the growth of cancer cells. Increased IGFBP-2 and IGFBP-5 production are observed in many human cancers, including prostate, breast, colorectal, non-small cell lung, glioblastoma, acute myeloid leukemia, acute lymphoblastic leukemia, neuroblastoma, and melanoma. The increased production of these proteins is linked to faster rates of cancer progression, treatment resistance, and shorter survival duration in humans.
Preclinical studies with human prostate and breast cancer cells have shown that reducing IGFBP-2 and IGFBP-5 production with OGX-225 sensitized these tumor types to hormone ablation therapy or chemotherapy and induced tumor cell death. We have completed IND enabling toxicology studies for OGX-225.
Collaboration Revenue
Revenue recognized to date was attributable to the upfront payment we received in the fourth quarter of 2009 pursuant to a Collaboration Agreement with Teva, as well as cash reimbursements from Teva for certain costs incurred by us under the clinical development plan. Our policy is to account for these reimbursements as collaboration revenue.
In April 2015, we and Teva entered into an agreement to terminate the Collaboration Agreement, or the Termination Agreement. Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, an amount equal to $27.0 million less approximately $3.8 million, which reduction represents a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and April 24, 2015, or Closing Date. Teva was permitted to deduct from the $3.0 million hold-back certain costs incurred after January 1, 2015 that arose after the Closing Date. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the hold-back had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount of the remaining hold-back in October 2015, representing one half of the then remaining amount six months after the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva. Teva is responsible for expenses related to custirsen incurred pursuant to the Collaboration Agreement through December 31, 2014. We will be responsible for certain custirsen-related expenses from and after January 1, 2015.
49
As a result of the termination of the Collaboration Agreement with Teva, we do not expect to earn any additional collaboration revenue beyond the amounts provided as advanced reimbursement for custirsen-related development expenses as set forth in the Termination Agreement. The advanced reimbursement payment made by Teva, as part of the Termination Agreement, was deferred and is being recognized as collaboration revenue on a dollar for dollar basis as costs are incurred as part the of continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin. Of the advance reimbursement received, we have incurred approximately $18.2 million for certain custirsen-related development costs since January 1, 2015 and recognized these amounts as Collaboration Revenue as of December 31, 2015.
Research and Development Expenses
Research and development, or R&D, expenses consist primarily of costs for clinical trials, contract manufacturing, personnel costs, milestone payments to third parties, facilities, regulatory activities, preclinical studies and allocations of other R&D-related costs. External expenses for clinical trials include fees paid to clinical research organizations, clinical trial site costs and patient treatment costs.
Currently, we manage our clinical trials through contract research organizations and independent medical investigators at their sites and at hospitals and expect this practice to continue. Through our clinical development programs, we are developing each of our product candidates in parallel for multiple disease indications. Due to the number of ongoing projects and our ability to utilize resources across several projects, we do not record or maintain information regarding the indirect operating costs incurred for our research and development programs on a program-specific basis. In addition, we believe that allocating costs on the basis of time incurred by our employees does not accurately reflect the actual costs of a project.
Several of our clinical trials have been supported by grant funding that was received directly by the hospitals and/or clinical investigators conducting the clinical trials as investigator-sponsored trials, thereby allowing us to complete these clinical trials at a lower cost to us.
Under the prior Collaboration Agreement with Teva, we were required to spend $30.0 million in direct and indirect development costs for the benefit of the custirsen development plan, such contribution to be funded by the upfront payment provided by Teva as an advanced reimbursement for our development expenses. In December 2012, we had spent the required $30.0 million in development costs related to custirsen. In accordance with the Termination Agreement, Teva was required to and did fund all additional expenses under the clinical development plan through December 31, 2014, after which date we took over responsibility for future custirsen-related costs following termination of our Collaboration Agreement. We do not owe Teva any development milestone payments or royalty payments on sales of custirsen, if any.
Final analyses of clinical trials involving our product candidates are dependent on and driven by timing of disease progression and/or survival events occurring and as a result we cannot estimate completion dates for development activities or when we might receive material net cash inflows from our R&D projects, if ever.
Our projects or intended R&D activities may be subject to change from time to time as we evaluate our R&D priorities and available resources.
General and Administrative Expenses
General and administrative, or G&A, expenses consist primarily of salaries and related costs for our personnel in executive, finance and accounting, corporate communications, human resources and other administrative functions, as well as consulting costs, including market research, business consulting and intellectual property. Other costs include professional fees for legal and auditing services, insurance and facility costs.
Warrant liability
The following is a summary of outstanding warrants to purchase common stock that are classified as liabilities at December 31, 2015:
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
Outstanding |
|
|
Exercise |
|
|
|
||
|
|
|
and |
|
|
price per |
|
|
|
||
|
|
|
Exercisable |
|
|
Share |
|
|
Expiration Date |
||
|
(1) Series A Warrants issued in July 2014 financing |
|
|
2,779,933 |
|
|
|
4.00 |
|
|
July 2019 |
|
(2) Series B Warrants issued in July 2014 financing |
|
|
670,269 |
|
|
|
4.00 |
|
|
July 2019 |
No warrants classified as liabilities were exercised during the years ended December 31, 2015 or 2014.
50
We reassess the fair value of the common stock warrants classified as liabilities at each reporting date utilizing a Black-Scholes pricing model. Inputs used in the pricing model include estimates of stock price volatility, expected warrant life and risk-free interest rate. The computation of expected volatility was based on the historical volatility of shares of our common stock for a period that coincides with the expected life of the warrants.
Results of Operations
Years Ended December 31, 2015, 2014 and 2013
Revenue
Revenue for the year ended December 31, 2015 decreased to $18.2 million, from $27.1 million for the year ended December 31, 2014 and decreased from $29.9 million for the year ended December 31, 2013. The advanced reimbursement payment made by Teva pursuant to the Termination Agreement was deferred and is being recognized as collaboration revenue on a dollar for dollar basis as costs are incurred as part of the continuing research and development activities related to custirsen. Revenue in all years was earned through our strategic collaboration with Teva. The decrease in 2015 as compared to 2014 was due primarily to lower collaboration revenue recognized for the reimbursement of expenses for the AFFINITY trial as a result of patients coming off treatment. This was partially offset by higher ENSPIRIT trial costs, which OncoGenex became responsible for pursuant to the Termination Agreement with Teva. Revenue recognized in 2015 is attributable to the advance reimbursement received in the second quarter of 2015, pursuant to the Termination Agreement with Teva, for research and development costs incurred by us related to the custirsen development program. The decrease in 2014 as compared with 2013 was due primarily to higher revenue earned from reimbursable purchases of combination drugs used in the AFFINITY trial during 2013.
Research and Development Expenses
Our research and development expenses for our clinical development programs were as follows (in thousands):
|
|
|
Year ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Clinical development programs: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Custirsen |
|
$ |
15,544 |
|
|
$ |
26,015 |
|
|
$ |
28,199 |
|
|
Apatorsen |
|
$ |
2,798 |
|
|
$ |
9,753 |
|
|
$ |
16,260 |
|
|
Other research and development |
|
$ |
6,766 |
|
|
$ |
10,456 |
|
|
$ |
10,858 |
|
|
Total research and development expenses |
|
$ |
25,108 |
|
|
$ |
46,224 |
|
|
$ |
55,317 |
|
Research and development expenses for the year ended December 31, 2015 decreased to $25.1 million, from $46.2 million for the year ended December 31, 2014 and decreased from $55.3 million for the year ended December 31, 2013. The decrease in 2015 as compared to 2014 was due primarily to lower clinical trial costs for the AFFINITY and Borealis-1 trials as a result of patients coming off treatment. This was partially offset by higher ENSPIRIT trial costs, which we became responsible for after the termination of our Collaboration Agreement with Teva. The decrease in 2014 as compared to 2013 was due primarily to lower clinical trial costs for Borealis-1 as a result of patients coming off treatment and fewer combination drug purchases for the AFFINITY trial in 2014.
General and Administrative Expenses
G&A expenses for the years ended December 31, 2015, 2014 and 2013 were $11.8 million, $10.6 million and $9.9 million, respectively. The increase in 2015 as compared to 2014 was primarily due to higher consulting and legal fees. This was partially offset by lower rent and facilities operating costs and lower employee related costs. The increase in 2014 compared to 2013 was primarily due to higher consulting fees.
Restructuring Gain
Restructuring gain for the years ended December 31, 2015, 2014 and 2013 was zero, $0.3 million and zero, respectively. We entered into a lease termination agreement with BMR-217TH Place LLC effective 2014 in relation to our previous Bothell facility. The termination of the lease resulted in a $3.5 million restructuring gain recorded in the fourth quarter of 2014, which was partially offset by a $3.2 million termination fee recognized in the same period.
51
Revaluation of Warrants
Recorded gains on the revaluation of our outstanding warrants for the years ended December 31, 2015, 2014 and 2013 were $1.9 million, $3.7 million and $3.2 million, respectively, which is included on our consolidated statement of loss as a gain on warrants. We revalue the warrants at each balance sheet date to fair value.
Liquidity and Capital Resources
We have incurred an accumulated deficit of $176.8 million through December 31, 2015, and we expect to incur substantial additional losses in the future as we continue or expand our R&D activities and other operations, as more fully described below. We have not generated any revenue from product sales to date, and we may not generate product sales revenue in the near future, if ever.
Our operations to date have been primarily funded through the sale of our equity securities and payments received from Teva. As of December 31, 2015, our cash, cash equivalents, and short-term investments increased to $55.2 million from $47.1 million as of December 31, 2014.
In April 2015, we and Teva terminated our Collaboration Agreement. Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen, an amount equal to $27.0 million less approximately $3.8 million, which reduction represented a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and the Closing Date. Teva was permitted to deduct from the $3.0 million hold-back certain custirsen-related costs incurred after January 1, 2015 that arose after the Closing Date. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the holdback had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount from the remaining hold-back in October 2015, representing one half of the then remaining amount six months from the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva.
Pursuant to the Termination Agreement, Teva remains responsible for expenses related to custirsen incurred pursuant to the Collaboration Agreement through December 31, 2014. We will be responsible for all custirsen-related expenses incurred from and after January 1, 2015. We do not owe Teva any development milestone payments or royalty payments on sales of custirsen, if any. As a result of the termination of the Collaboration Agreement, other than the advanced reimbursement for certain continuing research and development activities related to custirsen already received by us, and any amounts paid to us from the hold-back by Teva, if any, we will not receive any future cash reimbursements from Teva for certain costs incurred by us in connection with the clinical development of custirsen. Of the advance reimbursement received, we have incurred approximately $18.2 million for certain custirsen-related development costs between January 1, 2015 and December 31, 2015.
In April 2015, we and Lincoln Park Capital Fund, LLC, or LPC, entered into a Purchase Agreement, pursuant to which we had the right to sell to LPC up to $18.0 million in shares of our common stock, par value $0.001 per share, subject to certain limitations and conditions set forth in the Purchase Agreement. LPC initially purchased 956,938 Series A-1 Units at a purchase price of $2.09 per unit, for aggregate gross proceeds of $2.0 million. Each Series A-1 Unit consisted of (i) one share of common stock and (ii) one warrant to purchase one-quarter of a share of common stock at an exercise price of $2.40 per share. After the initial purchase, we had the right, from time to time, in our sole discretion and subject to certain conditions, to direct LPC to purchase additional shares of common stock having an aggregate value of $16.0 million. We directed LPC to purchase such additional shares as often as every business day over the 24-month term of the Purchase Agreement in increments of up to 125,000 shares of common stock, with such number of shares increasing as the closing sale price of our common stock increased. The purchase price of shares of common stock pursuant to the Purchase Agreement was based on prevailing market prices of common stock at the time of sale without any fixed discount, and we controlled the timing and amount of common stock sold to LPC. In addition, we had the right to direct LPC to purchase additional amounts as accelerated purchases if on the date of a regular purchase the closing sale price of the common stock is not below $1.50 per share. As consideration for entering into the Purchase Agreement, we issued to LPC 126,582 shares of common stock; no cash proceeds were received from the issuance of these shares.
From April 30, 2015 through August 13, 2015, we offered and sold 6,814,980 shares of our common stock pursuant to our Purchase Agreement with LPC. These sales resulted in gross proceeds to us of approximately $18.0 million and offering expenses of $0.4 million. As of August 13, 2015, no further amounts remained available for sale under this offering program.
52
In February 2016, we committed to a plan to reduce operating expenses, which included a workforce reduction of 11 employees, representing approximately 27% of our employees prior to the reduction. We estimate we will incur approximately $0.4 million in cash expenditures as a result of the workforce reduction, substantially all of which will be severance costs. We expect cost savings associated with the reduction of employees and consultants, together with the elimination of certain planned expenditures not required for the completion of ongoing trials, will extend our cash runway into the third quarter of 2017. Our currently planned operations are set forth below under the heading “Operating Capital and Capital Expenditure Requirements.”
Cash Flows
Operating Activities
For the years ended December 31, 2015, 2014 and 2013, net cash used in operating activities was $9.1 million, $17.3 million and $35.9 million, respectively. The decrease in cash used in operations in 2015 as compared to cash used for operations in 2014 was primarily attributable to a cash payment from Teva as an advance reimbursement for custirsen development costs associated with the Termination Agreement in 2015. The decrease in cash used in operations in 2014 as compared to 2013 is primarily attributable to an increase in cash reimbursements from Teva in 2014 as a result of us fulfilling our obligation of funding $30 million towards the development of custirsen, and the timing of payments for our clinical development activities.
Financing Activities
For the years ended December 31, 2015, 2014 and 2013 net cash provided by financing activities was $17.6 million, $25.2 million and $10,000, respectively. Net cash provided by financing activities for the year ended December 31, 2015 relates to proceeds received from the financing through our purchase agreement with LPC. Net cash provided by financing activities for the year ended December 31, 2014 was the result of proceeds from the underwritten registered direct offering completed in July 2014, the sale of shares of common stock through our “at the market” equity offering program and the exercise of stock options. Net cash provided by financing activities for the year ended December 31, 2013 was the result of proceeds from the exercise of stock options.
Investing Activities
Net cash used in investing activities for the year ended December 31, 2015 was $2.1 million. Net cash provided by investing activities for the years ended December 31, 2014 and 2013 was $5.4 million and $32.4 million, respectively. Net cash used in and provided by investing activities in all years was due to transactions involving marketable securities in the normal course of business.
Operating Capital and Capital Expenditure Requirements
Based on our current expectations, we believe that our cash, cash equivalents, and short-term investments will be sufficient to fund our currently planned operations into the third quarter of 2017. Depending on timing of enrollment or event-driven final analyses, the expected key milestones and activities are as follows:
|
|
• |
|
Custirsen |
|
|
• |
|
Announcing AFFINITY trial results, the phase 3 trial evaluating a survival benefit for custirsen in combination with cabazitaxel as second-line chemotherapy in approximately 630 patients with castrate-resistant prostate cancer. The final analysis for the intent-to-treat population is expected in the third quarter of 2016. |
|
|
• |
|
Announcing ENSPIRIT trial results, the phase 3 trial evaluating a survival benefit for custirsen in combination with docetaxel as second-line chemotherapy in approximately 700 patients with non-small cell lung cancer. The final survival analysis is expected in the first half of 2017. |
|
|
• |
|
Apatorsen |
|
|
• |
|
Announcing Borealis-2 trial results, an investigator-sponsored, randomized phase 2 trial evaluating apatorsen in combination with docetaxel treatment compared to docetaxel treatment alone in patients with advanced or metastatic bladder cancer. Final results are expected in the second half of 2016. |
|
|
• |
|
Announcing Spruce trial results for the overall survival endpoint, the investigator-sponsored, randomized, placebo-controlled phase 2 trial evaluating apatorsen treatment with carboplatin and pemetrexed chemotherapy in patients with previously untreated advanced non-squamous NSCLC. Results are expected in the second half of 2016. |
|
|
• |
|
Preparing an investigational new drug application for FDA submission regarding apatorsen via intravesical administration in combination with Bacillus Calmette-Guerin (BCG) treatment in patients with non-muscle invasive bladder cancer. |
53
Results from the custirsen and apatorsen trials may be released at a date that is beyond the period for which we currently project we have available cash resources. We have based this estimate on assumptions that may prove to be wrong, or we could utilize our available capital resources sooner than we currently expect. We would require additional funding to support our operations if we were to continue the AFFINITY or ENSPIRIT trials beyond their anticipated data result dates, spend capital on activities related to product launch, acquire or invest in other assets, conduct development activities with respect to our other product candidates beyond those development activities described above, including activities with respect to OGX-225 or unsuccessfully defend pending litigation, or if the clinical trials cost more than we anticipate or custirsen is successful in a phase 3 trial with no partnership. If we need to extend our cash availability or to conduct any such currently unplanned development activities, we would seek such necessary funding through the licensing or sale of certain of our product candidates, by executing a partnership or collaboration agreement, or through private or public offerings of our equity or debt. However, we can provide no assurance that such funding would be available to us on favorable terms, or at all.
Our future capital requirements will depend on many factors, including:
|
|
· |
timing, costs and results of clinical development, preclinical development and regulatory approvals; |
|
|
· |
our ability to obtain additional funding through a partnership or collaboration agreement with a third party or licenses of certain of our product candidates, or through private or public offerings of our equity or debt, or through sale of certain of our royalty rights; |
|
|
· |
our ongoing level of focus and efforts to develop and commercialize custirsen and apatorsen; |
|
|
· |
success of custirsen and apatorsen; |
|
|
· |
costs to defend, and results of, pending litigation; and |
|
|
· |
costs related to obtaining, defending and enforcing patents. |
Contractual Obligations
The following table summarizes our contractual obligations as of December 31, 2015 (in thousands):
|
|
|
Total |
|
|
Less than 1 year |
|
|
1-3 years |
|
|
3-5 years |
|
|
More than 5 years |
|
|||||
|
Bothell office operating lease (1) |
|
$ |
643 |
|
|
$ |
267 |
|
|
$ |
376 |
|
|
$ |
— |
|
|
$ |
— |
|
|
Vancouver office operating lease (2) |
|
$ |
62 |
|
|
$ |
62 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
UBC license maintenance fees (3) |
|
$ |
36 |
|
|
$ |
6 |
|
|
$ |
12 |
|
|
$ |
12 |
|
|
$ |
6 |
|
|
Leased equipment |
|
$ |
41 |
|
|
$ |
19 |
|
|
$ |
22 |
|
|
$ |
— |
|
|
$ |
— |
|
|
Total |
|
$ |
782 |
|
|
$ |
354 |
|
|
$ |
410 |
|
|
$ |
12 |
|
|
$ |
6 |
|
|
(1) |
This operating lease is effective May 1, 2015 and expires on April 30, 2018. |
|
(2) |
This operating lease expires in 2016. |
|
(3) |
We are obligated to pay an annual license maintenance fee of CAD$8,000 to UBC, which has been converted to US dollars based on the December 31, 2015 exchange rate of US$1.00 = CAD$1.384, and rounded to the nearest $1,000. |
Off-Balance Sheet Arrangements
We do not have any off-balance sheet financing arrangements at December 31, 2015.
Inflation
We do not believe that inflation has had a material effect on our business and results of operations during the periods presented.
Material Changes in Financial Condition
|
|
|
December 31, |
|
|||||
|
(in thousands) |
|
2015 |
|
|
2014 |
|
||
|
Total Assets |
|
$ |
58,209 |
|
|
$ |
56,291 |
|
|
Total Liabilities |
|
|
20,769 |
|
|
|
22,232 |
|
|
Total Equity |
|
|
37,440 |
|
|
|
34,059 |
|
54
The increase in assets at December 31, 2015 compared with December 31, 2014 was primarily due to an increase in cash as a result of the cash payment from Teva as an advance reimbursement for custirsen development costs associated with the Termination Agreement in 2015 and proceeds received from the financings under our purchase agreement with LPC. The decrease in liabilities at December 31, 2015 compared with December 31, 2014 is primarily due to lower clinical trial accruals associated with patient enrollment and treatment in the AFFINITY trial and our investigator sponsored trials evaluating apatorsen.
Critical Accounting Policies and Estimates
Use of Estimates
The preparation of consolidated financial statements in conformity with United States generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and notes thereto. Actual results could differ from these estimates. Estimates and assumptions principally relate to estimates of the fair value of our warrant liability, the initial fair value and forfeiture rates of stock options issued to employees and consultants, the estimated compensation cost on performance restricted stock unit awards and clinical trial and manufacturing accruals, estimated useful lives of property, plant and equipment and estimates and assumptions in contingent liabilities.
Cash Equivalents
We consider all highly liquid investments with an original maturity of three months or less to be cash equivalents, which we consider as available for sale and carry at fair value, with unrealized gains and losses, if any, reported as accumulated other comprehensive income or loss, which is a separate component of stockholders’ equity.
Short-Term Investments
Short-term investments consist of financial instruments purchased with an original maturity of greater than three months and less than one year. We consider our short-term investments as available-for-sale and carry them at fair value, with unrealized gains and losses except other than temporary losses, if any, reported as accumulated other comprehensive income or loss, which is a separate component of stockholders’ equity. Realized gains and losses on the sale of these securities are recognized in net income or loss. The cost of investments sold is based on the specific identification method.
Fair value of financial instruments
The fair value of our cash equivalents and marketable securities is based on quoted market prices and trade data for comparable securities. We determine the fair value of our warrant liability based on the Black-Scholes pricing model and using considerable judgment, including estimating stock price volatility and expected warrant life. Other financial instruments including amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities, accrued compensation and lease termination liability are carried at cost, which we believe approximates fair value because of the short-term maturities of these instruments.
Intellectual Property
The costs of acquiring intellectual property rights to be used in the research and development process, including licensing fees and milestone payments, are charged to research and development expense as incurred in situations where we have not identified an alternative future use for the acquired rights, and are capitalized in situations where we have identified an alternative future use. No costs associated with acquiring intellectual property rights have been capitalized to date. Costs of maintaining intellectual property rights are expensed as incurred.
Revenue Recognition
Revenue recognized to date is attributable to the upfront payment we received in the fourth quarter of 2009 pursuant to the collaboration agreement with Teva, as well as cash reimbursements from Teva for costs incurred by us under the clinical development plan. In April 2015, OncoGenex Technologies and Teva entered into an agreement, or the Termination Agreement, pursuant to which the Collaboration Agreement was terminated and we regained rights to custirsen.
Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, an amount equal to $27.0 million less approximately $3.8 million, which reduction represents a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and April 24, 2015, or Closing Date. Teva was permitted to deduct from the $3.0 million hold-back certain costs incurred after January 1, 2015 that arose after the Closing Date. Teva will be responsible for expenses related to custirsen incurred pursuant to the Collaboration Agreement through December 31, 2014. We will be responsible for certain custirsen-related expenses from and after January 1, 2015. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to
55
us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the holdback had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount from the remaining hold-back in October 2015, representing one half of the then remaining amount six months from the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva.
As a result of the termination of the Collaboration Agreement with Teva, we do not expect to earn any additional collaboration revenue beyond the amounts provided as advanced reimbursement for custirsen-related development expenses as set forth in the Termination Agreement. The advanced reimbursement payment made by Teva, as part of the Termination Agreement, was deferred and is being recognized as collaboration revenue on a dollar for dollar basis as costs are incurred as part the of continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin. Of the advance reimbursement received, we have incurred approximately $18.2 million for certain custirsen-related development costs since January 1, 2015 and recognized these amounts as Collaboration Revenue as of December 31, 2015.
Prior to the termination of the collaboration agreement, we and Teva shared certain custirsen-related development costs. We had spent the required $30 million in direct and indirect development costs, such as full-time equivalent (FTE) reimbursement for time incurred by our personnel for the benefit of the custirsen development plan. Teva funded all other expenses under the collaboration agreement including the three phase 3 clinical trials under the clinical development plan. On a quarterly basis Teva reimbursed all development expenses incurred in accordance with our clinical development plan. Our policy was to account for these reimbursements as Collaboration Revenue. For a summary description of the collaboration agreement with Teva see also Note 4.
The terminated collaboration agreement contained multiple elements and deliverables, and required evaluation pursuant to ASC 605-25, Multiple-Element Arrangements, or ASC 605-25. We evaluated the facts and circumstances of the collaboration agreement to determine whether we had obligations constituting deliverables under ASC 605-25. We concluded that we had multiple deliverables under the collaboration agreement, including deliverables relating to the grant of a technology license, and performance of manufacturing, regulatory and clinical development services in the U.S. and Canada, and estimated that the period in which it would perform those deliverables began in the fourth quarter of 2009 and was completed in the fourth quarter of 2012. Because we have been able to establish vendor specific objective evidence, or VSOE, of the fair value of the maintenance, regulatory, and clinical services, we concluded that these deliverables should be accounted as separate units of accounting under ASC 605-25. In establishing VSOE for the manufacturing, regulatory, and clinical development services, management relied on rates charged by other service providers providing similar development services.
As of December 31, 2012 we had recognized the entire $30 million allocated to the manufacturing, regulatory and clinical development services element as revenue on a proportional performance basis.
Because we were not able to reliably estimate the fair value of the technology license, we used the residual value approach to determine the amount of revenue to recognize. Based on this approach, we recognized $22 million in 2009 relating to this element.
Property and Equipment
Property and equipment assets are recorded at cost less accumulated depreciation. Depreciation expense on assets acquired under capital lease is recorded within depreciation expense. Depreciation is recorded on a straight-line basis over the following periods:
|
Computer equipment |
|
3 years |
|
Furniture and fixtures |
|
5 years |
|
Machinery and equipment |
|
5 - 10 years |
|
Leasehold improvements and equipment under capital lease |
|
Over the term of the lease |
Income Taxes
Income taxes are accounted for under the liability method. Deferred tax assets and liabilities are recognized for the differences between the carrying values of assets and liabilities and their respective income tax bases and for operating losses and tax credit carry forwards. A valuation allowance is provided for the portion of deferred tax assets that is more likely than not to be unrealized. Deferred tax assets and liabilities are measured using the enacted tax rates and laws.
Scientific Research and Development Tax Credits
The benefits of tax credits for scientific research and development expenditures are recognized in the year the qualifying expenditure is made provided there is reasonable assurance of recoverability. The tax credits recorded are based on our estimates of amounts
56
expected to be recovered and are subject to audit by taxation authorities. The non-refundable tax credit reduces the tax provision; however, no reduction to the tax provision has been recorded to date as we record a full valuation allowance. All qualifying expenditures are eligible for non-refundable tax credits only.
Research and Development Costs
Research and development costs are expensed as incurred, net of related refundable investment tax credits, with the exception of non-refundable advanced payments for goods or services to be used in future research and development, which are capitalized in accordance with ASC 730, “Research and Development” and included within Prepaid Expenses or Other Assets depending on when the assets will be utilized.
Clinical trial expenses are a component of research and development costs. These expenses include fees paid to contract research organizations and investigators and other service providers, which conduct certain product development activities on our behalf. We use an accrual basis of accounting, based upon estimates of the amount of service completed. In the event payments differ from the amount of service completed, prepaid expense or accrued liabilities amounts are adjusted on the balance sheet. These expenses are based on estimates of the work performed under service agreements, milestones achieved, patient enrollment and experience with similar contracts. We monitor each of these factors to the extent possible and adjusts estimates accordingly.
Stock-Based Compensation
Effective January 1, 2006, we adopted the fair value recognition provisions of the ASC 718, “Stock Compensation”, using the modified prospective method with respect to options granted to employees and directors. Under this transition method, compensation cost is recognized in the financial statements beginning with the effective date for all share-based payments granted after January 1, 2006 and for all awards granted prior to but not yet vested as of January 1, 2006. The expense is amortized on a straight-line basis over the graded vesting period.
Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four-year period. We also granted restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision or the occurrence of other events that may have caused the awards to accelerate and vest.
Segment Information
We follow the requirements of ASC 280, “Segment Reporting.” We have one operating segment, dedicated to the development and commercialization of new cancer therapies, with operations located in Canada and the United States.
Comprehensive Income (Loss)
Comprehensive income (loss) is comprised of net income (loss) and other comprehensive income (loss). Other comprehensive income (loss) consists of unrealized gains and losses on our available-for-sale marketable securities. We report the components of comprehensive loss in the statement of stockholders’ equity.
Loss per Common Share
Basic loss per common share is computed using the weighted average number of common shares outstanding during the period. Diluted loss per common share is computed in accordance with the treasury stock method. The effect of potentially issuable common shares from outstanding stock options, restricted stock unit awards and warrants are anti-dilutive for all periods presented.
Warrants
We account for warrants pursuant to the authoritative guidance on accounting for derivative financial instruments indexed to, and potentially settled in, a company’s own stock, on the understanding that in compliance with applicable securities laws, the warrants require the issuance of registered securities upon exercise and therefore do not sufficiently preclude an implied right to net cash settlement. We classify warrants on the consolidated balance sheet as a liability which is revalued at each balance sheet date subsequent to the initial issuance. We also have warrants classified as equity and these are not reassessed for their fair value at the end of each reporting period. Warrants classified as equity are initially measured at their fair value and recognized as part of stockholders’ equity. Determining the appropriate fair-value model and calculating the fair value of registered warrants requires considerable
57
judgment, including estimating stock price volatility and expected warrant life. The computation of expected volatility was based on the historical volatility of shares of our common stock for a period that coincides with the expected life of the warrants. A small change in the estimates used may have a relatively large change in the estimated valuation. We use the Black-Scholes pricing model to value the warrants. Changes in the fair value of the warrants classified as liabilities are reflected in the consolidated statement of loss as gain (loss) on revaluation of warrants.
Foreign Currency Translation
Our functional and reporting currency is the U.S. dollar. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates.
The functional currency of our foreign subsidiary is the U.S. dollar. For this foreign operation, assets and liabilities denominated in other than U.S. dollars are translated at the period-end rates for monetary assets and liabilities and historical rates for non-monetary assets and liabilities. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates. Gains and losses from this translation are recognized in the consolidated statement of loss.
Pending Adoption of Recent Accounting Pronouncements
On February 2016, the Financial Accounting Standards Board ("FASB") issued its new leases standard, ASU No. 2016-02, Leases (Topic 842) ("ASU 2016-02"). ASU 2016-02 is aimed at putting most leases on lessees’ balance sheets, but it would also change aspects of lessor accounting. ASU 2016-02 is effective for public business entities for annual periods beginning after December 15, 2018 and interim periods within that year. This standard is expected to have a significant impact on our current accounting for our lease arrangements, particularly our current operating lease arrangements, as well as, disclosures. We are currently evaluating the impact of adoption on its financial position and results from operations.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes. The standard requires that deferred tax liabilities and assets be classified as noncurrent in a classified statement of financial position. Entities are currently required to separate deferred income tax liabilities and assets into current and noncurrent amounts in a classified statement of financial position. The amendments, which require non-current presentation only (by jurisdiction), are effective for financial statements issued for annual periods beginning after December 15, 2016 with earlier application permitted as of the beginning of an interim or annual reporting period. The guidance is to be applied either prospectively to all deferred tax liabilities and assets or retrospectively to all periods presented. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-17 on our consolidated financial statements and related disclosures.
In February 2015, the FASB issued ASU 2015-02, Consolidation (Topic 810) — Amendments to the Consolidation Analysis. ASU 2015-02 eliminates the deferral of FAS 167 and makes changes to both the variable interest model and the voting model. For public business entities, the guidance is effective for annual and interim periods beginning after 15 December 2015. For nonpublic business entities, it is effective for annual periods beginning after 15 December 2016, and interim periods beginning after 15 December 2017. Early adoption is permitted for annual and interim periods. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-02 on our consolidated financial statements and related disclosures.
In January 2015, the FASB issued ASU 2015-01, Income Statement—Extraordinary and Unusual Items (Subtopic 225-20): Simplifying Income Statement Presentation by Eliminating the Concept of Extraordinary Items. ASU 2015-01 eliminates the concept of reporting extraordinary items, but retains current presentation and disclosure requirements for an event or transaction that is of an unusual nature or of a type that indicates infrequency of occurrence. Transactions that meet both criteria would now also follow such presentation and disclosure requirements. For all entities, the guidance is effective for annual periods, and interim periods within those annual periods, beginning after 15 December 2015. Early adoption is permitted; however, adoption must occur at the beginning of an annual period and can be applied prospectively or retrospectively. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-01 on our consolidated financial statements and related disclosures.
In August 2014, the Financial Accounting Standards Board, or FASB issued Accounting Standards Updated, or ASU No. 2014-15, Presentation of Financial Statements-Going Concern (Subtopic 2015-40) (ASU 2014-15). ASU 2014-15 provides guidance to U.S. GAAP about management’s responsibility to evaluate whether there is a substantial doubt about an entity’s ability to continue as a going concern and to provide related footnote disclosures. This new rule requires management to assess an entity’s ability to continue as a going concern by incorporating and expanding upon certain principles currently in the U.S. auditing standards. Specifically, ASU 2014-15 (1) defines the term substantial doubt, (2) requires an evaluation of every reporting period including interim periods, (3) provides principles for considering the mitigating effect of management’s plans, (5) requires an express statement and other disclosures when substantial doubt is not alleviated, and (6) requires an assessment for a period of one year after the date that the financial statements are issued (or available to be issued). This guidance is effective for annual periods ending after December 15, 2016. We are currently in the process of evaluating the impact of adoption of ASU No. 2014. Depending on our capital resources and
58
forecasted expenses at the time of adoption, the impact of ASU No. 2014-15 could have an impact on our consolidated financial statements and related disclosures.
In May 2014, the FASB, issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606): Revenue from Contracts with Customers, which guidance in this update will supersede the revenue recognition requirements in Topic 605, Revenue Recognition, and most industry-specific guidance when it becomes effective. ASU No. 2014-09 affects any entity that enters into contracts with customers to transfer goods or services or enters into contracts for the transfer of nonfinancial assets unless those contracts are within the scope of other standards. The core principal of ASU No. 2014-09 is that a company will recognize revenue when it transfers promised goods or services to customers in an amount that reflects the consideration to which the company expects to be entitled in exchange for those goods or services. In doing so, companies will need to use more judgment and make more estimates than under current guidance. These may include identifying performance obligations in the contract, estimating the amount of variable consideration to include in the transaction price and allocating the transaction price to each separate performance obligation. ASU No. 2014-09 is effective for annual reporting periods beginning after December 15, 2017, including interim periods within that reporting period, which will be our fiscal year 2018 (or December 31, 2018), and entities can transition to the standard either retrospectively or as a cumulative-effect adjustment as of the date of adoption. Early adoption is permitted. We are currently in the process of evaluating the impact of adoption of ASU No. 2014-09 on our consolidated financial statements and related disclosures.
Recently Adopted Accounting Policies
In July 2013, the FASB issued ASU No. 2013-11, Income Taxes (Topic 740): Presentation of an Unrecognized Tax Benefit When a Net Operating Loss Carryforward, a Similar Tax Loss, or a Tax Credit Carryforward Exists (a consensus of the FASB Emerging Issues Task Force) (ASU 2013-11), which provides clarification on the financial statement presentation of unrecognized tax benefits. ASU 2013-11 specifies that an unrecognized tax benefit (or a portion thereof) shall be presented in the financial statements as a reduction to a deferred tax asset when a net operating loss carryforward, a similar tax loss, or a tax credit carryforward exists. If such deferred tax asset is not available at the reporting date to settle additional income taxes resulting from the disallowance of a tax position, or the entity does not plan to use the deferred tax asset for such purpose given the option, the unrecognized tax benefit shall be presented in the financial statements as a liability and shall not be combined with deferred tax assets. The amendments in ASU 2013-11 are effective for fiscal years (and interim periods within those years) beginning after December 15, 2013, with early adoption permitted. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In February 2013, the FASB issued Accounting Standards Updates, or ASU, No. 2013-02, “Other Comprehensive Income.” This ASU requires an entity to provide information about the amounts reclassified out of accumulated other comprehensive income by component. In addition, an entity is required to present, either on the face of the statement where net income is presented or in the notes, significant amounts reclassified out of accumulated other comprehensive income by the respective line items of net income but only if the amount reclassified is required under generally accepted accounting principles in the United States, or U.S. GAAP, to be reclassified to net income in its entirety in the same reporting period. For other amounts that are not required under U.S. GAAP to be reclassified in their entirety to net income, an entity is required to cross-reference to other disclosures required under U.S. GAAP that provide additional detail about those amounts. We adopted ASU 2013-02 for our fiscal year ended December 31, 2013. The adoption of this standard did not have a significant impact on our financial position or results of operations.
Interest Rate Risk
Interest rate risk is the risk that the fair values and future cash flows of financial instruments will fluctuate because of the changes in market interest rates. We invest our cash in a variety of financial instruments, primarily in short-term bank deposits, money market funds, and domestic and foreign commercial paper and government securities. These investments are denominated in U.S. dollars, and we monitor our exposure to interest rate changes is monitored. We have very limited interest rate risk due to the few assets or liabilities subject to fluctuations in interest rates. Our investment portfolio includes only marketable securities with active secondary or resale markets to help ensure portfolio liquidity. Due to the nature of our highly liquid marketable securities, a change in interest rates would not materially change the fair market value. We have estimated the effect on our portfolio of a hypothetical increase in interest rates by one percent to be a reduction of $0.4 million in the fair value of our investments as of December 31, 2015.
Foreign Currency Exchange Risk
We are exposed to risks associated with foreign currency transactions on certain contracts and payroll expenses related to our Canadian subsidiary, OncoGenex Technologies, denominated in Canadian dollars and we have not hedged these amounts. As our unhedged foreign currency transactions fluctuate, our earnings might be negatively affected. Accordingly, changes in the value of the U.S. dollar relative to the Canadian dollar might have an adverse effect on our reported results of operations and financial condition, and fluctuations in exchange rates might harm our reported results and accounts from period to period. We have estimated the effect
59
on our reported results of operations of a hypothetical increase of 10 percent in the exchange rate of the Canadian dollar against the U.S. dollar to be $0.2 million for the year ended December 31, 2015.
60
INDEX TO FINANCIAL STATEMENTS:
61
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
OncoGenex Pharmaceuticals, Inc.
We have audited the accompanying consolidated balance sheets of OncoGenex Pharmaceuticals, Inc. (the “Company”) as of December 31, 2015 and 2014, and the related consolidated statements of loss and comprehensive loss, stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2015. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of OncoGenex Pharmaceuticals, Inc. at December 31, 2015 and 2014, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2015, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), OncoGenex Pharmaceuticals, Inc.’s internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 Framework) and our report dated March 9, 2016 expressed an unqualified opinion thereon.
|
Vancouver, Canada |
|
|
/s/ ERNST & YOUNG LLP |
|
|
March 9, 2016 |
|
|
Chartered Professional Accountants |
|
62
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
OncoGenex Pharmaceuticals, Inc.
We have audited OncoGenex Pharmaceuticals, Inc.’s (the “Company”) internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 Framework) (the COSO criteria). OncoGenex Pharmaceuticals, Inc.’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying “Management’s Report on Internal Control over Financial Reporting”. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, OncoGenex Pharmaceuticals, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2015, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of OncoGenex Pharmaceuticals, Inc. as of December 31, 2015 and 2014, and the related consolidated statements of loss and comprehensive loss, stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2015 and our report dated March 9, 2016 expressed an unqualified opinion thereon.
|
Vancouver, Canada |
|
|
/s/ ERNST & YOUNG LLP |
|
|
March 9, 2016 |
|
|
Chartered Professional Accountants |
|
63
OncoGenex Pharmaceuticals, Inc.
(In thousands, except per share and share amounts)
|
|
|
December 31, |
|
|||||
|
|
|
2015 |
|
|
2014 |
|
||
|
ASSETS |
|
|
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
|
|
Cash and cash equivalents [note 5] |
|
$ |
34,310 |
|
|
$ |
27,897 |
|
|
Restricted cash [note 5] |
|
|
— |
|
|
|
251 |
|
|
Short-term investments [note 5] |
|
|
20,876 |
|
|
|
19,160 |
|
|
Interest receivable |
|
|
111 |
|
|
|
113 |
|
|
Amounts receivable |
|
|
14 |
|
|
|
5,676 |
|
|
Prepaid expenses |
|
|
1,987 |
|
|
|
2,165 |
|
|
Other current assets [note 8] |
|
|
— |
|
|
|
499 |
|
|
Total current assets |
|
|
57,298 |
|
|
|
55,761 |
|
|
Restricted cash [note 5] |
|
|
272 |
|
|
|
— |
|
|
Property and equipment, net [note 6] |
|
|
602 |
|
|
|
257 |
|
|
Other assets [note 8] |
|
|
37 |
|
|
|
273 |
|
|
Total assets |
|
$ |
58,209 |
|
|
$ |
56,291 |
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY |
|
|
|
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
1,343 |
|
|
$ |
72 |
|
|
Accrued liabilities other |
|
|
641 |
|
|
|
863 |
|
|
Accrued clinical liabilities |
|
|
9,966 |
|
|
|
13,462 |
|
|
Accrued compensation |
|
|
1,267 |
|
|
|
1,333 |
|
|
Current portion of long-term obligations [note 12] |
|
|
52 |
|
|
|
236 |
|
|
Lease termination liability [note 7] |
|
|
1,250 |
|
|
|
3,250 |
|
|
Deferred collaboration revenue [note 4] |
|
|
5,040 |
|
|
|
— |
|
|
Warrant liability [note 5 and note 10] |
|
|
1,105 |
|
|
|
3,002 |
|
|
Total current liabilities |
|
|
20,664 |
|
|
|
22,218 |
|
|
Long-term obligations, less current portion [note 12] |
|
|
105 |
|
|
|
14 |
|
|
Total liabilities |
|
|
20,769 |
|
|
|
22,232 |
|
|
Commitments and contingencies [note 4 and note 12] |
|
|
|
|
|
|
|
|
|
Stockholders' equity: |
|
|
|
|
|
|
|
|
|
Common stock, $0.001 par value, 75,000,000 shares authorized, 29,846,991 and 22,630,652 issued at December 31, 2015 and December 31, 2014, respectively, and 29,812,998 and 22,621,426 outstanding at December 31, 2015 and December 31, 2014, respectively |
|
|
29 |
|
|
|
22 |
|
|
Additional paid-in capital |
|
|
211,590 |
|
|
|
191,373 |
|
|
Accumulated deficit |
|
|
(176,811 |
) |
|
|
(159,958 |
) |
|
Accumulated other comprehensive income |
|
|
2,632 |
|
|
|
2,622 |
|
|
Total stockholders' equity |
|
|
37,440 |
|
|
|
34,059 |
|
|
Total liabilities and stockholders' equity |
|
$ |
58,209 |
|
|
$ |
56,291 |
|
|
Subsequent events [note 14] |
|
|
|
|
|
|
|
|
See accompanying notes.
64
OncoGenex Pharmaceuticals, Inc.
Consolidated Statements of Loss and Comprehensive Loss
(In thousands, except per share and share amounts)
|
|
|
Year Ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
COLLABORATION REVENUE (note 4) |
|
$ |
18,160 |
|
|
$ |
27,116 |
|
|
$ |
29,882 |
|
|
EXPENSES |
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
25,108 |
|
|
|
46,224 |
|
|
|
55,317 |
|
|
General and administrative |
|
|
11,805 |
|
|
|
10,625 |
|
|
|
9,892 |
|
|
Restructuring gain |
|
|
— |
|
|
|
(267 |
) |
|
|
— |
|
|
Total operating expenses |
|
|
36,913 |
|
|
|
56,582 |
|
|
|
65,209 |
|
|
OTHER INCOME (EXPENSE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest income |
|
|
119 |
|
|
|
35 |
|
|
|
150 |
|
|
Other income (expense) |
|
|
(64 |
) |
|
|
(19 |
) |
|
|
120 |
|
|
Warrant issuance costs |
|
|
— |
|
|
|
(531 |
) |
|
|
— |
|
|
Gain on warrants |
|
|
1,897 |
|
|
|
3,741 |
|
|
|
3,208 |
|
|
Total other income |
|
|
1,952 |
|
|
|
3,226 |
|
|
|
3,478 |
|
|
Net loss |
|
$ |
(16,801 |
) |
|
$ |
(26,240 |
) |
|
$ |
(31,849 |
) |
|
OTHER COMPREHENSIVE INCOME |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net unrealized gain (loss) on securities |
|
|
10 |
|
|
|
(21 |
) |
|
|
6 |
|
|
Total other comprehensive income (loss) |
|
|
10 |
|
|
|
(21 |
) |
|
|
6 |
|
|
Comprehensive loss |
|
$ |
(16,791 |
) |
|
$ |
(26,261 |
) |
|
$ |
(31,843 |
) |
|
Basic and diluted net loss per common share [note 10 [h]] |
|
$ |
(0.64 |
) |
|
$ |
(1.45 |
) |
|
$ |
(2.17 |
) |
|
Shares used in computation of basic and diluted net loss per common share [note 10 [h]] |
|
|
26,147,344 |
|
|
|
18,098,799 |
|
|
|
14,683,389 |
|
See accompanying notes.
65
OncoGenex Pharmaceuticals, Inc.
Consolidated Statements of Stockholders’ Equity
(In thousands, except share amounts)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
|
Other |
|
|
|
|
|
|
Total |
|
|||
|
|
|
Common Stock |
|
|
Paid-in |
|
|
Comprehensive |
|
|
Accumulated |
|
|
Stockholders’ |
|
|||||||||
|
|
|
Shares |
|
|
Amount |
|
|
Capital |
|
|
Income (Loss) |
|
|
Deficit |
|
|
Equity |
|
||||||
|
Balance, January 1, 2013 |
|
|
14,656,916 |
|
|
$ |
15 |
|
|
$ |
165,395 |
|
|
$ |
2,637 |
|
|
$ |
(101,840 |
) |
|
$ |
66,207 |
|
|
Stock-based compensation expense |
|
|
— |
|
|
|
— |
|
|
|
2,837 |
|
|
|
— |
|
|
|
— |
|
|
|
2,837 |
|
|
Stock option exercises |
|
|
3,475 |
|
|
|
— |
|
|
|
10 |
|
|
|
— |
|
|
|
— |
|
|
|
10 |
|
|
Restricted Stock Unit Settlements |
|
|
47,495 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(31,849 |
) |
|
|
(31,849 |
) |
|
Other comprehensive income (loss) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
6 |
|
|
|
— |
|
|
|
6 |
|
|
Balance, December 31, 2013 |
|
|
14,707,886 |
|
|
|
15 |
|
|
|
168,242 |
|
|
|
2,643 |
|
|
|
(133,689 |
) |
|
|
37,211 |
|
|
Stock-based compensation expense |
|
|
— |
|
|
|
— |
|
|
|
3,860 |
|
|
|
— |
|
|
|
— |
|
|
|
3,860 |
|
|
Stock option exercises |
|
|
10,000 |
|
|
|
— |
|
|
|
30 |
|
|
|
— |
|
|
|
— |
|
|
|
30 |
|
|
Restricted Stock Unit Settlements |
|
|
53,971 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Performance Restricted Stock Unit Settlements |
|
|
149,177 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Performance Restricted Stock Unit Settlements withheld and retired to treasury |
|
|
(9,226 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(29 |
) |
|
|
(29 |
) |
|
Shares issued - ATM Financing |
|
|
809,214 |
|
|
|
— |
|
|
|
2,860 |
|
|
|
— |
|
|
|
— |
|
|
|
2,860 |
|
|
Shares issued in July 2014 Financing |
|
|
5,559,866 |
|
|
|
6 |
|
|
|
16,369 |
|
|
|
— |
|
|
|
— |
|
|
|
16,375 |
|
|
Warrant Exercises |
|
|
1,340,538 |
|
|
|
1 |
|
|
|
12 |
|
|
|
— |
|
|
|
— |
|
|
|
13 |
|
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(26,240 |
) |
|
|
(26,240 |
) |
|
Other comprehensive income (loss) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(21 |
) |
|
|
— |
|
|
|
(21 |
) |
|
Balance, December 31, 2014 |
|
|
22,621,426 |
|
|
|
22 |
|
|
|
191,373 |
|
|
|
2,622 |
|
|
|
(159,958 |
) |
|
|
34,059 |
|
|
Stock-based compensation expense |
|
|
— |
|
|
|
— |
|
|
|
2,328 |
|
|
|
— |
|
|
|
— |
|
|
|
2,328 |
|
|
Stock option exercises |
|
|
5,359 |
|
|
|
— |
|
|
|
14 |
|
|
|
— |
|
|
|
— |
|
|
|
14 |
|
|
Restricted Stock Unit Settlements |
|
|
186,991 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Performance Restricted Stock Unit Settlements |
|
|
82,410 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Performance Restricted Stock Unit Settlements withheld and retired to treasury |
|
|
(24,750 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(52 |
) |
|
|
(52 |
) |
|
Shares issues - Lincoln Park Capital |
|
|
6,941,562 |
|
|
|
7 |
|
|
|
17,875 |
|
|
|
|
|
|
|
|
|
|
|
17,882 |
|
|
Net loss |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(16,801 |
) |
|
|
(16,801 |
) |
|
Other comprehensive income (loss) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
10 |
|
|
|
— |
|
|
|
10 |
|
|
Balance, December 31, 2015 |
|
|
29,812,998 |
|
|
$ |
29 |
|
|
$ |
211,590 |
|
|
$ |
2,632 |
|
|
$ |
(176,811 |
) |
|
$ |
37,440 |
|
See accompanying notes.
66
OncoGenex Pharmaceuticals, Inc.
Consolidated Statements of Cash Flows
(In thousands)
|
|
|
Year Ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Operating Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(16,801 |
) |
|
$ |
(26,240 |
) |
|
$ |
(31,849 |
) |
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gain on warrants |
|
|
(1,897 |
) |
|
|
(3,741 |
) |
|
|
(3,208 |
) |
|
Warrant issuance costs |
|
|
|
|
|
|
531 |
|
|
|
— |
|
|
Depreciation |
|
|
244 |
|
|
|
223 |
|
|
|
227 |
|
|
Stock-based compensation [note10[c]] |
|
|
2,328 |
|
|
|
3,860 |
|
|
|
2,834 |
|
|
Restructuring gain [note 7] |
|
|
— |
|
|
|
(3,517 |
) |
|
|
— |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest receivable |
|
|
2 |
|
|
|
105 |
|
|
|
109 |
|
|
Amounts receivable |
|
|
5,662 |
|
|
|
2,981 |
|
|
|
(7,943 |
) |
|
Prepaid expenses and other assets |
|
|
1,167 |
|
|
|
3,944 |
|
|
|
(1,974 |
) |
|
Accounts payable |
|
|
1,271 |
|
|
|
(67 |
) |
|
|
(1,190 |
) |
|
Accrued liabilities other |
|
|
(222 |
) |
|
|
363 |
|
|
|
41 |
|
|
Accrued clinical liabilities |
|
|
(3,714 |
) |
|
|
2,178 |
|
|
|
7,563 |
|
|
Accrued compensation |
|
|
(66 |
) |
|
|
(372 |
) |
|
|
164 |
|
|
Restricted cash |
|
|
(21 |
) |
|
|
63 |
|
|
|
— |
|
|
Excess lease liability [note 7] |
|
|
(194 |
) |
|
|
(785 |
) |
|
|
(680 |
) |
|
Lease obligation |
|
|
100 |
|
|
|
(84 |
) |
|
|
(21 |
) |
|
Lease termination fees [note 12] |
|
|
(2,000 |
) |
|
|
3,250 |
|
|
|
— |
|
|
Deferred collaboration revenue |
|
|
5,040 |
|
|
|
— |
|
|
|
— |
|
|
Net cash used in operating activities |
|
|
(9,101 |
) |
|
|
(17,308 |
) |
|
|
(35,927 |
) |
|
Financing Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Proceeds from the exercise of stock options |
|
|
14 |
|
|
|
30 |
|
|
|
10 |
|
|
Proceeds from ATM Financing, net of issuance costs |
|
|
17,629 |
|
|
|
2,874 |
|
|
|
— |
|
|
Taxes paid related to net share settlement of equity awards |
|
|
(52 |
) |
|
|
(29 |
) |
|
|
— |
|
|
Issuance of common shares, net of share issuance costs |
|
|
— |
|
|
|
22,372 |
|
|
|
— |
|
|
Net cash provided by financing activities |
|
|
17,591 |
|
|
|
25,247 |
|
|
|
10 |
|
|
Investing Activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Purchase of investments |
|
|
(24,368 |
) |
|
|
(19,446 |
) |
|
|
(31,696 |
) |
|
Proceeds from sale of investments |
|
|
1,003 |
|
|
|
— |
|
|
|
1,000 |
|
|
Proceeds from maturities of investments |
|
|
21,659 |
|
|
|
24,894 |
|
|
|
63,375 |
|
|
Purchase of property and equipment |
|
|
(371 |
) |
|
|
(82 |
) |
|
|
(253 |
) |
|
Net cash provided by (used in) investing activities |
|
|
(2,077 |
) |
|
|
5,366 |
|
|
|
32,426 |
|
|
Effect of exchange rate changes on cash |
|
|
— |
|
|
|
(1 |
) |
|
|
9 |
|
|
Net increase (decrease) in cash and cash equivalents |
|
|
6,413 |
|
|
|
13,304 |
|
|
|
(3,482 |
) |
|
Cash and cash equivalents at beginning of year |
|
|
27,897 |
|
|
|
14,593 |
|
|
|
18,075 |
|
|
Cash and cash equivalents at end of year |
|
$ |
34,310 |
|
|
$ |
27,897 |
|
|
$ |
14,593 |
|
|
Supplemental Disclosure of Cash Flow Information: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Property and equipment received and accrued but not yet paid |
|
$ |
218 |
|
|
$ |
— |
|
|
$ |
— |
|
|
Property and equipment acquired under lease obligation |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
24 |
|
See accompanying notes.
67
OncoGenex Pharmaceuticals, Inc.
Notes to Consolidated Financial Statements
(In thousands, except per share and share amounts)
1. NATURE OF BUSINESS AND BASIS OF PRESENTATION
OncoGenex Pharmaceuticals, Inc. (referred to as “OncoGenex,” “we,” “us,” or “our”) is committed to the development and commercialization of new therapies that address treatment resistance in cancer patients. We were incorporated in the state of Delaware and are headquartered in Bothell, Washington and have a subsidiary in Vancouver, British Columbia.
Basis of Presentation
The accompanying consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States. The consolidated financial statements include the accounts of OncoGenex Pharmaceuticals, Inc. and its wholly owned subsidiary OncoGenex Technologies, Inc.
Liquidity
We have historically experienced recurring losses from operations that have generated an accumulated deficit of $176.8 million through December 31, 2015. At December 31, 2015, we had cash, cash equivalents and short-term investments of $55.2 million.
2. ACCOUNTING POLICIES
Significant Accounting Policies
Use of Estimates
The preparation of consolidated financial statements in conformity with United States generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and notes thereto. Actual results could differ from these estimates. Estimates and assumptions principally relate to estimates of the fair value of our warrant liability, the initial fair value and forfeiture rates of stock options issued to employees and consultants, the estimated compensation cost on performance restricted stock unit awards and clinical trial and manufacturing accruals, estimated useful lives of property, plant and equipment and estimates and assumptions in contingent liabilities.
Cash Equivalents
We consider all highly liquid investments with an original maturity of three months or less to be cash equivalents, which we consider as available for sale and carry at fair value, with unrealized gains and losses, if any, reported as accumulated other comprehensive income or loss, which is a separate component of stockholders’ equity.
Short-Term Investments
Short-term investments consist of financial instruments purchased with an original maturity of greater than three months and less than one year. We consider our short-term investments as available-for-sale and carry them at fair value, with unrealized gains and losses except other than temporary losses, if any, reported as accumulated other comprehensive income or loss, which is a separate component of stockholders’ equity. Realized gains and losses on the sale of these securities are recognized in net income or loss. The cost of investments sold is based on the specific identification method.
Fair value of financial instruments
The fair value of our cash equivalents and marketable securities is based on quoted market prices and trade data for comparable securities. We determine the fair value of our warrant liability based on the Black-Scholes pricing model and using considerable judgment, including estimating stock price volatility and expected warrant life. Other financial instruments including amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities, accrued compensation and lease termination liability are carried at cost, which we believe approximates fair value because of the short-term maturities of these instruments.
Intellectual Property
The costs of acquiring intellectual property rights to be used in the research and development process, including licensing fees and milestone payments, are charged to research and development expense as incurred in situations where we have not identified an
68
alternative future use for the acquired rights, and are capitalized in situations where we have identified an alternative future use. No costs associated with acquiring intellectual property rights have been capitalized to date. Costs of maintaining intellectual property rights are expensed as incurred.
Revenue Recognition
Revenue recognized to date is attributable to the upfront payment we received in the fourth quarter of 2009 pursuant to the collaboration agreement with Teva, as well as cash reimbursements from Teva for costs incurred by us under the clinical development plan. In April 2015, OncoGenex Technologies and Teva entered into an agreement, or the Termination Agreement, pursuant to which the Collaboration Agreement was terminated and we regained rights to custirsen.
Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, an amount equal to $27.0 million less approximately $3.8 million, which reduction represents a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and April 24, 2015, or Closing Date. Teva was permitted to deduct from the $3.0 million hold-back certain costs incurred after January 1, 2015 that arose after the Closing Date. Teva will be responsible for expenses related to custirsen incurred pursuant to the Collaboration Agreement through December 31, 2014. We will be responsible for certain custirsen-related expenses from and after January 1, 2015. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the holdback had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount from the remaining hold-back in October 2015, representing one half of the then remaining amount six months from the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva.
As a result of the termination of the Collaboration Agreement with Teva, we do not expect to earn any additional collaboration revenue beyond the amounts provided as advanced reimbursement for custirsen-related development expenses as set forth in the Termination Agreement. The advanced reimbursement payment made by Teva, as part of the Termination Agreement, was deferred and is being recognized as collaboration revenue on a dollar for dollar basis as costs are incurred as part the of continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin. Of the advance reimbursement received, we have incurred approximately $18.2 million for certain custirsen-related development costs since January 1, 2015 and recognized these amounts as Collaboration Revenue as of December 31, 2015.
Prior to the termination of the collaboration agreement, we and Teva shared certain custirsen-related development costs. We had spent the required $30 million in direct and indirect development costs, such as full-time equivalent (FTE) reimbursement for time incurred by our personnel for the benefit of the custirsen development plan. Teva funded all other expenses under the collaboration agreement including the three phase 3 clinical trials under the clinical development plan. On a quarterly basis Teva reimbursed all development expenses incurred in accordance with our clinical development plan. Our policy was to account for these reimbursements as Collaboration Revenue. For a summary description of the collaboration agreement with Teva see also Note 4.
The terminated collaboration agreement contained multiple elements and deliverables, and required evaluation pursuant to ASC 605-25, Multiple-Element Arrangements, or ASC 605-25. We evaluated the facts and circumstances of the collaboration agreement to determine whether we had obligations constituting deliverables under ASC 605-25. We concluded that we had multiple deliverables under the collaboration agreement, including deliverables relating to the grant of a technology license, and performance of manufacturing, regulatory and clinical development services in the U.S. and Canada, and estimated that the period in which it would perform those deliverables began in the fourth quarter of 2009 and was completed in the fourth quarter of 2012. Because we have been able to establish vendor specific objective evidence, or VSOE, of the fair value of the maintenance, regulatory, and clinical services, we concluded that these deliverables should be accounted as separate units of accounting under ASC 605-25. In establishing VSOE for the manufacturing, regulatory, and clinical development services, management relied on rates charged by other service providers providing similar development services.
As of December 31, 2012 we had recognized the entire $30 million allocated to the manufacturing, regulatory and clinical development services element as revenue on a proportional performance basis.
Because we were not able to reliably estimate the fair value of the technology license, we used the residual value approach to determine the amount of revenue to recognize. Based on this approach, we recognized $22 million in 2009 relating to this element.
69
Property and Equipment
Property and equipment assets are recorded at cost less accumulated depreciation. Depreciation expense on assets acquired under capital lease is recorded within depreciation expense. Depreciation is recorded on a straight-line basis over the following periods:
|
Computer equipment |
|
3 years |
|
Furniture and fixtures |
|
5 years |
|
Machinery and equipment |
|
5 - 10 years |
|
Leasehold improvements and equipment under capital lease |
|
Over the term of the lease |
Income Taxes
Income taxes are accounted for under the liability method. Deferred tax assets and liabilities are recognized for the differences between the carrying values of assets and liabilities and their respective income tax bases and for operating losses and tax credit carry forwards. A valuation allowance is provided for the portion of deferred tax assets that is more likely than not to be unrealized. Deferred tax assets and liabilities are measured using the enacted tax rates and laws.
Scientific Research and Development Tax Credits
The benefits of tax credits for scientific research and development expenditures are recognized in the year the qualifying expenditure is made provided there is reasonable assurance of recoverability. The tax credits recorded are based on our estimates of amounts expected to be recovered and are subject to audit by taxation authorities. The non-refundable tax credit reduces the tax provision; however, no reduction to the tax provision has been recorded to date as we record a full valuation allowance. All qualifying expenditures are eligible for non-refundable tax credits only.
Research and Development Costs
Research and development costs are expensed as incurred, net of related refundable investment tax credits, with the exception of non-refundable advanced payments for goods or services to be used in future research and development, which are capitalized in accordance with ASC 730, “Research and Development” and included within Prepaid Expenses or Other Assets depending on when the assets will be utilized.
Clinical trial expenses are a component of research and development costs. These expenses include fees paid to contract research organizations and investigators and other service providers, which conduct certain product development activities on our behalf. We use an accrual basis of accounting, based upon estimates of the amount of service completed. In the event payments differ from the amount of service completed, prepaid expense or accrued liabilities amounts are adjusted on the balance sheet. These expenses are based on estimates of the work performed under service agreements, milestones achieved, patient enrollment and experience with similar contracts. We monitor each of these factors to the extent possible and adjusts estimates accordingly.
Stock-Based Compensation
Effective January 1, 2006, we adopted the fair value recognition provisions of the ASC 718, “Stock Compensation”, using the modified prospective method with respect to options granted to employees and directors. Under this transition method, compensation cost is recognized in the financial statements beginning with the effective date for all share-based payments granted after January 1, 2006 and for all awards granted prior to but not yet vested as of January 1, 2006. The expense is amortized on a straight-line basis over the graded vesting period.
Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four-year period. We also granted restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision or the occurrence of other events that may have caused the awards to accelerate and vest.
Segment Information
We follow the requirements of ASC 280, “Segment Reporting.” We have one operating segment, dedicated to the development and commercialization of new cancer therapies, with operations located in Canada and the United States.
70
Comprehensive Income (Loss)
Comprehensive income (loss) is comprised of net income (loss) and other comprehensive income (loss). Other comprehensive income (loss) consists of unrealized gains and losses on our available-for-sale marketable securities. We report the components of comprehensive loss in the statement of stockholders’ equity.
Loss per Common Share
Basic loss per common share is computed using the weighted average number of common shares outstanding during the period. Diluted loss per common share is computed in accordance with the treasury stock method. The effect of potentially issuable common shares from outstanding stock options, restricted stock unit awards and warrants are anti-dilutive for all periods presented.
Warrants
We account for warrants pursuant to the authoritative guidance on accounting for derivative financial instruments indexed to, and potentially settled in, a company’s own stock, on the understanding that in compliance with applicable securities laws, the warrants require the issuance of registered securities upon exercise and therefore do not sufficiently preclude an implied right to net cash settlement. We classify warrants on the consolidated balance sheet as a liability which is revalued at each balance sheet date subsequent to the initial issuance. We also have warrants classified as equity and these are not reassessed for their fair value at the end of each reporting period. Warrants classified as equity are initially measured at their fair value and recognized as part of stockholders’ equity. Determining the appropriate fair-value model and calculating the fair value of registered warrants requires considerable judgment, including estimating stock price volatility and expected warrant life. The computation of expected volatility was based on the historical volatility of shares of our common stock for a period that coincides with the expected life of the warrants. A small change in the estimates used may have a relatively large change in the estimated valuation. We use the Black-Scholes pricing model to value the warrants. Changes in the fair value of the warrants classified as liabilities are reflected in the consolidated statement of loss as gain (loss) on revaluation of warrants.
Foreign Currency Translation
Our functional and reporting currency is the U.S. dollar. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates.
The functional currency of our foreign subsidiary is the U.S. dollar. For this foreign operation, assets and liabilities denominated in other than U.S. dollars are translated at the period-end rates for monetary assets and liabilities and historical rates for non-monetary assets and liabilities. Revenues and expenses denominated in other than U.S. dollars are translated at average monthly rates. Gains and losses from this translation are recognized in the consolidated statement of loss.
Pending Adoption of Recent Accounting Pronouncements
On February 2016, the Financial Accounting Standards Board ("FASB") issued its new leases standard, ASU No. 2016-02, Leases (Topic 842) ("ASU 2016-02"). ASU 2016-02 is aimed at putting most leases on lessees’ balance sheets, but it would also change aspects of lessor accounting. ASU 2016-02 is effective for public business entities for annual periods beginning after December 15, 2018 and interim periods within that year. This standard is expected to have a significant impact on our current accounting for our lease arrangements, particularly our current operating lease arrangements, as well as, disclosures. We are currently evaluating the impact of adoption on its financial position and results from operations.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes. The standard requires that deferred tax liabilities and assets be classified as noncurrent in a classified statement of financial position. Entities are currently required to separate deferred income tax liabilities and assets into current and noncurrent amounts in a classified statement of financial position. The amendments, which require non-current presentation only (by jurisdiction), are effective for financial statements issued for annual periods beginning after December 15, 2016 with earlier application permitted as of the beginning of an interim or annual reporting period. The guidance is to be applied either prospectively to all deferred tax liabilities and assets or retrospectively to all periods presented. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-17 on our consolidated financial statements and related disclosures
In February 2015, the FASB issued ASU 2015-02, Consolidation (Topic 810) — Amendments to the Consolidation Analysis. ASU 2015-02 eliminates the deferral of FAS 167 and makes changes to both the variable interest model and the voting model. For public business entities, the guidance is effective for annual and interim periods beginning after 15 December 2015. For nonpublic business entities, it is effective for annual periods beginning after 15 December 2016, and interim periods beginning after 15 December 2017. Early adoption is permitted for annual and interim periods. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-02 on our consolidated financial statements and related disclosures.
71
In January 2015, the FASB issued ASU 2015-01, Income Statement—Extraordinary and Unusual Items (Subtopic 225-20): Simplifying Income Statement Presentation by Eliminating the Concept of Extraordinary Items. ASU 2015-01 eliminates the concept of reporting extraordinary items, but retains current presentation and disclosure requirements for an event or transaction that is of an unusual nature or of a type that indicates infrequency of occurrence. Transactions that meet both criteria would now also follow such presentation and disclosure requirements. For all entities, the guidance is effective for annual periods, and interim periods within those annual periods, beginning after 15 December 2015. Early adoption is permitted; however, adoption must occur at the beginning of an annual period and can be applied prospectively or retrospectively. We are currently in the process of evaluating the impact of adoption of ASU No. 2015-01 on our consolidated financial statements and related disclosures.
In August 2014, the Financial Accounting Standards Board, or FASB issued Accounting Standards Updated, or ASU No. 2014-15, Presentation of Financial Statements-Going Concern (Subtopic 2015-40) (ASU 2014-15). ASU 2014-15 provides guidance to U.S. GAAP about management’s responsibility to evaluate whether there is a substantial doubt about an entity’s ability to continue as a going concern and to provide related footnote disclosures. This new rule requires management to assess an entity’s ability to continue as a going concern by incorporating and expanding upon certain principles currently in the U.S. auditing standards. Specifically, ASU 2014-15 (1) defines the term substantial doubt, (2) requires an evaluation of every reporting period including interim periods, (3) provides principles for considering the mitigating effect of management’s plans, (5) requires an express statement and other disclosures when substantial doubt is not alleviated, and (6) requires an assessment for a period of one year after the date that the financial statements are issued (or available to be issued). This guidance is effective for annual periods ending after December 15, 2016. We are currently in the process of evaluating the impact of adoption of ASU No. 2014. Depending on our capital resources and forecasted expenses at the time of adoption, the impact of ASU No. 2014-15 could have an impact on our consolidated financial statements and related disclosures.
In May 2014, the FASB, issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606): Revenue from Contracts with Customers, which guidance in this update will supersede the revenue recognition requirements in Topic 605, Revenue Recognition, and most industry-specific guidance when it becomes effective. ASU No. 2014-09 affects any entity that enters into contracts with customers to transfer goods or services or enters into contracts for the transfer of nonfinancial assets unless those contracts are within the scope of other standards. The core principal of ASU No. 2014-09 is that a company will recognize revenue when it transfers promised goods or services to customers in an amount that reflects the consideration to which the company expects to be entitled in exchange for those goods or services. In doing so, companies will need to use more judgment and make more estimates than under current guidance. These may include identifying performance obligations in the contract, estimating the amount of variable consideration to include in the transaction price and allocating the transaction price to each separate performance obligation. ASU No. 2014-09 is effective for annual reporting periods beginning after December 15, 2017, including interim periods within that reporting period, which will be our fiscal year 2018 (or December 31, 2018), and entities can transition to the standard either retrospectively or as a cumulative-effect adjustment as of the date of adoption. Early adoption is permitted. We are currently in the process of evaluating the impact of adoption of ASU No. 2014-09 on our consolidated financial statements and related disclosures.
Recently Adopted Accounting Policies
In July 2013, the FASB issued ASU No. 2013-11, Income Taxes (Topic 740): Presentation of an Unrecognized Tax Benefit When a Net Operating Loss Carryforward, a Similar Tax Loss, or a Tax Credit Carryforward Exists (a consensus of the FASB Emerging Issues Task Force) (ASU 2013-11), which provides clarification on the financial statement presentation of unrecognized tax benefits. ASU 2013-11 specifies that an unrecognized tax benefit (or a portion thereof) shall be presented in the financial statements as a reduction to a deferred tax asset when a net operating loss carryforward, a similar tax loss, or a tax credit carryforward exists. If such deferred tax asset is not available at the reporting date to settle additional income taxes resulting from the disallowance of a tax position, or the entity does not plan to use the deferred tax asset for such purpose given the option, the unrecognized tax benefit shall be presented in the financial statements as a liability and shall not be combined with deferred tax assets. The amendments in ASU 2013-11 are effective for fiscal years (and interim periods within those years) beginning after December 15, 2013, with early adoption permitted. The adoption of this standard did not have a significant impact on our financial position or results of operations.
In February 2013, the FASB issued Accounting Standards Updates, or ASU, No. 2013-02, “Other Comprehensive Income.” This ASU requires an entity to provide information about the amounts reclassified out of accumulated other comprehensive income by component. In addition, an entity is required to present, either on the face of the statement where net income is presented or in the notes, significant amounts reclassified out of accumulated other comprehensive income by the respective line items of net income but only if the amount reclassified is required under generally accepted accounting principles in the United States, or U.S. GAAP, to be reclassified to net income in its entirety in the same reporting period. For other amounts that are not required under U.S. GAAP to be reclassified in their entirety to net income, an entity is required to cross-reference to other disclosures required under U.S. GAAP that provide additional detail about those amounts. We adopted ASU 2013-02 for our fiscal year ended December 31, 2013. The adoption of this standard did not have a significant impact on our financial position or results of operations.
72
3. FINANCIAL INSTRUMENTS AND RISK
For certain of our financial instruments, including cash and cash equivalents, amounts receivable, accounts payable, accrued liabilities other, accrued clinical liabilities, accrued compensation and lease termination liability carrying values approximate fair value due to their short-term nature. Our cash equivalents and short-term investments are recorded at fair value.
Financial risk is the risk to our results of operations that arises from fluctuations in interest rates and foreign exchange rates and the degree of volatility of these rates as well as credit risk associated with the financial stability of the issuers of the financial instruments. Foreign exchange rate risk arises as a portion of our investments which finance operations and a portion of our expenses are denominated in other than U.S. dollars.
We invest our excess cash in accordance with investment guidelines, which limit our credit exposure to any one financial institution or corporation other than securities issued by the U.S. government. We only invest in A (or equivalent) rated securities with maturities of one year or less. These securities generally mature within one year or less and in some cases are not collateralized. At December 31, 2015, the average days to maturity of our portfolio of cash equivalents and marketable securities was 61 days (December 31, 2014 – 174 days). We do not use derivative instruments to hedge against any of these financial risks.
4. COLLABORATION AGREEMENT
In December 2009, we, through our wholly-owned subsidiary, OncoGenex Technologies, entered into a collaboration agreement, or Collaboration Agreement, with Teva Pharmaceutical Industries Ltd., or Teva, for the development and global commercialization of custirsen (and related compounds), a pharmaceutical compound designed to inhibit the production of clusterin, a protein we believe is associated with cancer treatment resistance, or the Licensed Product. In December 2014, we and Teva agreed to terminate the Collaboration Agreement upon entry into a termination agreement. In April 2015, OncoGenex Technologies and Teva entered into an agreement, or the Termination Agreement, pursuant to which the Collaboration Agreement was terminated and we regained rights to custirsen.
Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen, an amount equal to $27.0 million less approximately $3.8 million, which reduction represented a hold-back amount of $3.0 million and $0.8 million for certain third-party expenses incurred by Teva between January 1, 2015 and April 24, 2015, or Closing Date. Teva was permitted to deduct from the $3.0 million hold-back certain costs incurred after January 1, 2015 that arose after the Closing Date. Teva will be responsible for expenses related to custirsen incurred pursuant to the Collaboration Agreement through December 31, 2014. We will be responsible for certain custirsen-related expenses from and after January 1, 2015. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the holdback had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount from the remaining hold-back in October 2015, representing one half of the then remaining amount six months from the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva.
In accordance with the Termination Agreement, Teva transferred certain third-party agreements for the ENSPIRIT study and custirsen development activities to us on the Closing Date. If any additional historical third-party agreements are discovered after the Closing Date and are used to conduct the ENSPIRIT study, then Teva will use commercially reasonable effort to assign such agreements to us and will be responsible for any costs invoiced under such agreements in excess of an aggregate of $0.1 million. We will be responsible for the initial $0.1 million of costs under such agreements.
All licenses granted by us to Teva under the Collaboration Agreement were terminated as of the Closing Date. In addition, Teva assigned to us certain patent applications related to custirsen and abandoned certain other patent applications as requested by us. Furthermore, Teva granted to us and our affiliates an exclusive license (except as to Teva and its affiliates) to any know-how created under and during the term of the Collaboration Agreement to develop, manufacture and commercialize custirsen and certain other antisense inhibitors of clusterin, as set forth in more detail in the Termination Agreement. Teva additionally granted to us and our affiliates a non-exclusive license to any intellectual property owned by or licensed to Teva and its affiliates, whether as of the Closing Date or thereafter, to develop, manufacture and commercialize custirsen, subject to certain limitations. Teva also agreed not to challenge the patentability, validity or enforceability of certain of our patents, and agreed not to file any patent applications covering custirsen or any antisense inhibitor of clusterin for 18 months after the Closing Date. We are responsible for any such expenses incurred from and after January 1, 2015. We do not owe Teva any development milestone payments or royalty payments on sales of custirsen, if any.
As part of the termination, Teva assigned to us the investigational new drug application for custirsen and submitted amendments, on a country-by-country basis, transferring sponsorship of the ENSPIRIT study to us. In July 2015, we became the sole trial sponsor for the ENSPIRIT study in all countries.
73
We and Teva released each other from all claims related to the Collaboration Agreement. In addition, we agreed to indemnify Teva and its affiliates against any third-party claims attributable to the development and commercialization of custirsen prior to the execution of the Collaboration Agreement and after the Closing Date, and any third-party claims attributable to the conduct of the AFFINITY study. Teva agreed to indemnify us and our affiliates against any third-party claims attributable to the development of custirsen during the period between the execution of the Collaboration Agreement and the Closing Date, but excluding the AFFINITY study. The parties’ indemnity obligations cover, among other things, third-party claims brought by current or former patients in the relevant studies and patient product liability claims.
Revenue for the year ended December 31, 2015 was $18.2 million, which consists of partial recognition of deferred collaboration revenue representing our efforts in the development of custirsen. As of December 31, 2015, a remaining balance of $5.0 million of the advanced reimbursement payment was recorded in deferred collaboration revenue. The advanced reimbursement payment made by Teva, as part of the Termination Agreement, was deferred and will be recognized as collaboration revenue on a dollar for dollar basis as costs are incurred as part of the continuing research and development activities related to custirsen.
Ionis and UBC License Agreements
Pursuant to the terms of the agreements with Ionis and UBC, we anticipate we will pay royalties to third-parties of 4.0% to 8.0% of net sales, unless our royalties are adjusted for competition from generic compounds, in which case royalties to third parties will also be subject to adjustment on a country-by-country basis. Certain third-party royalties are tiered based on the royalty rate received by us. Minimum royalty rates payable by us assume certain third-party royalties are not paid at the time that the Licensed Product is marketed due to the expiration of patents held by such third parties. Maximum royalty rates assume all third-party royalty rates currently in effect continue in effect at the time the Licensed Product is marketed. We did not make any royalty payments to Ionis in 2015. In addition, pursuant to the terms of the agreement with Ionis, we are required to pay to Ionis up to 20% of all non-royalty revenue (defined to mean revenue not based on net sales of products) we receive from third parties. Pursuant to the terms of agreement with UBC, we are required to pay low single digit royalties on milestones and the revenue from sales of custirsen. We did not make any royalty or milestone payments to UBC under the terms of the agreement in 2015.
In May and November 2015, we received communications from Ionis requesting payment of 30% of the $23.2 million paid by Teva under the Termination Agreement, as well as 30% of any amounts paid by Teva upon release of the $3.0 million holdback amount. In January 2016, Ionis filed a lawsuit and claims that OncoGenex Technologies is in breach of the license agreement for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva in connection with the termination of the Collaboration Agreement. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the license agreement. We do not believe that any payments are due to Ionis. Under the Ionis license agreement, no payment is due to Ionis on any consideration that we receive for the reimbursement for research and development activities. The amounts paid or payable by Teva under the Termination Agreement constitute an advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, and therefore, no payments are owed to Ionis. We intend to vigorously defend the lawsuit and, based on our preliminary review, we believe we have valid defenses.
Amendment to Ionis and UBC License Agreements
To facilitate the execution and performance of our prior Collaboration Agreement with Teva, we and Ionis agreed to amend the Ionis License Agreement and we and UBC agreed to amend the UBC License Agreement, in each case, effective December 19 and December 20, 2009, respectively.
The amendment to the Ionis License Agreement provides, among other things, that if we are the subject of a change of control with a third party, where the surviving company immediately following such change of control has the right to develop and sell the product, then (i) a milestone payment of $20.0 million will be due and payable to Ionis 21 days following the first commercial sale of the product in the United States; and (ii) unless such surviving entity had previously sublicensed the product and a royalty rate payable to Ionis by us has been established, the applicable royalty rate payable to Ionis will thereafter be the maximum amount payable under the Ionis License Agreement. Any non-royalty milestone amounts previously paid will be credited toward the $20.0 million milestone if not already paid. As a result of the $10.0 million milestone payment payable to Ionis in relation to the Collaboration Agreement entered into with Teva in 2009, the remaining amount owing in the event of change of control discussed above is a maximum of $10.0 million.
5. FAIR VALUE MEASUREMENTS
Assets and liabilities recorded at fair value in the balance sheets are categorized based upon the level of judgment associated with the inputs used to measure their fair value. For certain of our financial instruments including amounts receivable and accounts payable the carrying values approximate fair value due to their short-term nature.
74
ASC 820 “Fair Value Measurements and Disclosures,” specifies a hierarchy of valuation techniques based on whether the inputs to those valuation techniques are observable or unobservable. In accordance with ASC 820, these inputs are summarized in the three broad level listed below:
|
|
· |
Level 1 – Quoted prices in active markets for identical securities. |
|
|
· |
Level 2 – Other significant inputs that are observable through corroboration with market data (including quoted prices in active markets for similar securities). |
|
|
· |
Level 3 – Significant unobservable inputs that reflect management’s best estimate of what market participants would use in pricing the asset or liability. |
As quoted prices in active markets are not readily available for certain financial instruments, we obtain estimates for the fair value of financial instruments through third-party pricing service providers.
In determining the appropriate levels, we performed a detailed analysis of the assets and liabilities that are subject to ASC 820.
We invest our excess cash in accordance with investment guidelines that limit the credit exposure to any one financial institution other than securities issued by the U.S. Government. These securities are not collateralized and mature within one year.
A description of the valuation techniques applied to our financial instruments measured at fair value on a recurring basis follows.
Financial Instruments
Cash
Significant amounts of cash are held on deposit with large well established U.S. and Canadian financial institutions.
U.S. Government and Agency Securities
U.S. Government Securities U.S. government securities are valued using quoted market prices. Valuation adjustments are not applied. Accordingly, U.S. government securities are categorized in Level 1 of the fair value hierarchy.
U.S. Agency Securities U.S. agency securities are comprised of two main categories consisting of callable and non-callable agency issued debt securities. Non-callable agency issued debt securities are generally valued using quoted market prices. Callable agency issued debt securities are valued by benchmarking model-derived prices to quoted market prices and trade data for identical or comparable securities. Actively traded non-callable agency issued debt securities are categorized in Level 1 of the fair value hierarchy. Callable agency issued debt securities are categorized in Level 2 of the fair value hierarchy.
Corporate and Other Debt
Corporate Bonds and Commercial Paper The fair value of corporate bonds and commercial paper is estimated using recently executed transactions, market price quotations (where observable), bond spreads or credit default swap spreads adjusted for any basis difference between cash and derivative instruments. The spread data used are for the same maturity as the bond. If the spread data does not reference the issuer, then data that reference a comparable issuer are used. When observable price quotations are not available, fair value is determined based on cash flow models with yield curves, bond or single name credit default swap spreads and recovery rates based on collateral values as significant inputs. Corporate bonds and commercial paper are generally categorized in Level 2 of the fair value hierarchy; in instances where prices, spreads or any of the other aforementioned key inputs are unobservable, they are categorized in Level 3 of the hierarchy.
Warrants
As of December 31, 2015, we recorded a $1.1 million warrant liability. We reassess the fair value of the common stock warrants classified as liabilities at each reporting date utilizing a Black-Scholes pricing model. Inputs used in the pricing model include estimates of stock price volatility, expected warrant life and risk-free interest rate. The computation of expected volatility is based on the historical volatility of shares of our common stock for a period that coincides with the expected life of the warrants that are classified as liabilities. Warrants that are classified as liabilities are categorized in Level 3 of the fair value hierarchy. A small change in the estimates used may have a relatively large change in the estimated valuation. Warrants that are classified as equity are not considered liabilities and therefore are not reassessed for their fair values at each reporting date.
75
The following table presents the changes in fair value of our total Level 3 financial liabilities for the year ended December 31, 2015. During the twelve months ended December 31, 2015, no common stock warrants were issued that were classified as liabilities (in thousands):
|
|
|
Liability at |
|
|
|
|
|
|
Unrealized |
|
|
Liability at |
|
|||
|
|
|
December 31, |
|
|
Issuance of |
|
|
Gain on |
|
|
December 31, |
|
||||
|
|
|
2014 |
|
|
Warrants |
|
|
warrants |
|
|
2015 |
|
||||
|
Warrant liability |
|
$ |
3,002 |
|
|
$ |
- |
|
|
$ |
(1,897 |
) |
|
$ |
1,105 |
|
The following table presents information about our assets and liabilities that are measured at fair value on a recurring basis, and indicates the fair value hierarchy of the valuation techniques we utilized to determine such fair value (in thousands):
|
December 31, 2015 |
|
Level 1 |
|
|
Level 2 |
|
|
Level 3 |
|
|
Total |
|
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
$ |
14,034 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
14,034 |
|
|
Money market securities (cash equivalents) |
|
|
20,276 |
|
|
|
— |
|
|
|
— |
|
|
|
20,276 |
|
|
Restricted cash (Note 12) |
|
|
272 |
|
|
|
— |
|
|
|
— |
|
|
|
272 |
|
|
Corporate bonds and commercial paper |
|
|
— |
|
|
|
20,876 |
|
|
|
— |
|
|
|
20,876 |
|
|
Total assets |
|
$ |
34,582 |
|
|
$ |
20,876 |
|
|
$ |
— |
|
|
$ |
55,458 |
|
|
Liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Warrants |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
1,105 |
|
|
$ |
1,105 |
|
|
December 31, 2014 |
|
Level 1 |
|
|
Level 2 |
|
|
Level 3 |
|
|
Total |
|
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
$ |
16,481 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
16,481 |
|
|
Money market securities (cash equivalents) |
|
|
11,416 |
|
|
|
— |
|
|
|
— |
|
|
|
11,416 |
|
|
Restricted cash (Note 12) |
|
|
251 |
|
|
|
— |
|
|
|
— |
|
|
|
251 |
|
|
Corporate bonds and commercial paper |
|
|
— |
|
|
|
19,160 |
|
|
|
— |
|
|
|
19,160 |
|
|
Total assets |
|
$ |
28,148 |
|
|
$ |
19,160 |
|
|
$ |
— |
|
|
$ |
47,308 |
|
|
Liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Warrants |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
3,002 |
|
|
$ |
3,002 |
|
Cash and cash equivalents and short term investments (in thousands):
|
|
|
|
|
|
|
Gross |
|
|
Gross |
|
|
|
|
|
||
|
|
|
Amortized |
|
|
Unrealized |
|
|
Unrealized |
|
|
Estimated |
|
||||
|
December 31, 2015 |
|
Cost |
|
|
Gains |
|
|
Losses |
|
|
Fair Value |
|
||||
|
Cash |
|
$ |
14,034 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
14,034 |
|
|
Money market securities |
|
|
20,276 |
|
|
|
— |
|
|
|
— |
|
|
|
20,276 |
|
|
Total cash and cash equivalents |
|
$ |
34,310 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
34,310 |
|
|
Money market securities (restricted cash) |
|
|
272 |
|
|
|
— |
|
|
|
— |
|
|
|
272 |
|
|
Total restricted cash |
|
$ |
272 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
272 |
|
|
Corporate bonds and commercial paper |
|
|
20,885 |
|
|
|
— |
|
|
|
(9 |
) |
|
|
20,876 |
|
|
Total short-term investments |
|
$ |
20,885 |
|
|
$ |
— |
|
|
$ |
(9 |
) |
|
$ |
20,876 |
|
|
|
|
|
|
|
|
Gross |
|
|
Gross |
|
|
|
|
|
||
|
|
|
Amortized |
|
|
Unrealized |
|
|
Unrealized |
|
|
Estimated |
|
||||
|
December 31, 2014 |
|
Cost |
|
|
Gains |
|
|
Losses |
|
|
Fair Value |
|
||||
|
Cash |
|
$ |
16,481 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
16,481 |
|
|
Money market securities |
|
|
11,416 |
|
|
|
— |
|
|
|
— |
|
|
|
11,416 |
|
|
Total cash and cash equivalents |
|
$ |
27,897 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
27,897 |
|
|
Money market securities (restricted cash) |
|
|
251 |
|
|
|
— |
|
|
|
— |
|
|
|
251 |
|
|
Total restricted cash |
|
$ |
251 |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
251 |
|
|
Corporate bonds and commercial paper |
|
|
19,179 |
|
|
|
1 |
|
|
|
(20 |
) |
|
|
19,160 |
|
|
Total short-term investments |
|
$ |
19,179 |
|
|
$ |
1 |
|
|
$ |
(20 |
) |
|
$ |
19,160 |
|
Our gross realized gains and losses on sales of available-for-sale securities were not material for the years ended December 31, 2015 and 2014.
76
All securities included in cash and cash equivalents have maturities of 90 days or less at the time of purchase. All securities included in short-term investments have maturities of within one year of the balance sheet date. The cost of securities sold is based on the specific identification method.
We only invest in A (or equivalent) rated securities with maturities of one year or less. We do not believe that there are any other than temporary impairments related to our investment in marketable securities at December 31, 2015, given the quality of the investment portfolio, its short-term nature, and subsequent proceeds collected on sale of securities that reached maturity.
6. PROPERTY AND EQUIPMENT
Property and equipment consisted of the following (in thousands):
|
|
|
|
|
|
|
Accumulated |
|
|
Net Book |
|
||
|
|
|
Cost |
|
|
Depreciation |
|
|
Value |
|
|||
|
December 31, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Computer equipment |
|
$ |
628 |
|
|
$ |
490 |
|
|
$ |
138 |
|
|
Furniture and fixtures |
|
|
172 |
|
|
|
163 |
|
|
|
9 |
|
|
Machinery and equipment |
|
|
218 |
|
|
|
1 |
|
|
|
217 |
|
|
Leasehold improvements |
|
|
257 |
|
|
|
99 |
|
|
|
158 |
|
|
Computer software |
|
|
494 |
|
|
|
425 |
|
|
|
69 |
|
|
Equipment under capital lease |
|
|
114 |
|
|
|
103 |
|
|
|
11 |
|
|
Total property and equipment |
|
$ |
1,883 |
|
|
$ |
1,281 |
|
|
$ |
602 |
|
|
December 31, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Computer equipment |
|
$ |
493 |
|
|
$ |
395 |
|
|
$ |
98 |
|
|
Furniture and fixtures |
|
|
170 |
|
|
|
151 |
|
|
|
19 |
|
|
Leasehold improvements |
|
|
55 |
|
|
|
55 |
|
|
|
— |
|
|
Computer software |
|
|
462 |
|
|
|
342 |
|
|
|
120 |
|
|
Equipment under capital lease |
|
|
114 |
|
|
|
94 |
|
|
|
20 |
|
|
Total property and equipment |
|
$ |
1,294 |
|
|
$ |
1,037 |
|
|
$ |
257 |
|
7. EXCESS LEASE LIABILITY
On August 21, 2008, Sonus Pharmaceuticals, Inc., or Sonus, completed a transaction (“the Arrangement”) with OncoGenex Technologies Inc., or OncoGenex Technologies, whereby Sonus acquired all of the outstanding preferred shares, common shares and convertible debentures of OncoGenex Technologies. Sonus then changed its name to OncoGenex Pharmaceuticals, Inc. Prior to the Arrangement, Sonus entered into a non-cancellable lease arrangement for office space located in Bothell, Washington, which is considered to be in excess of our current requirements. The liability was computed as the present value of the difference between the remaining lease payments due less the estimate of net sublease income and expenses and had been accounted for in accordance with ASC 805-20, “Business Combinations -Identifiable Assets and Liabilities, and Any Non-controlling Interest.” Effective 2014, we entered into a Lease Termination Agreement with the landlord for the office space in Bothell such that the lease terminated effective March 1, 2015. Under the Lease Termination Agreement, we paid BMR-217TH Place LLC (“BMR”) a $2.0 million termination fee on the Termination Date. We will also pay BMR an additional termination fee of $1.3 million within 30 days after we (i) meet the primary endpoint for our phase 3 clinical trial for the treatment of second line metastatic CRPC with custirsen and (ii) close a transaction or transactions pursuant to which we receive funding in an aggregate amount of at least $20.0 million. As a result of the Lease Termination Agreement, we have recorded the lease termination fees and have made an adjustment to remove the excess lease liability.
8. OTHER ASSETS
Other assets include prepaid amounts related to clinical trials that will not be utilized in the next 12 months and deposits paid for office space in accordance with the terms of the operating lease agreements.
77
9. INCOME TAX
[a] The reconciliation of income tax attributable to operations computed at the statutory tax rate to income tax expense is as follows. OncoGenex Technologies, a Canadian corporation, which is subject to combined Canadian federal and provincial statutory tax rates for December 31, 2015, 2014, and 2013 of 26.0%, 26.0%, and 25.75%, respectively. Following the reverse takeover by OncoGenex Technologies of Sonus Pharmaceuticals, Inc. (which subsequently changed its name to OncoGenex Pharmaceuticals, Inc.) in 2008, OncoGenex Technologies became a wholly owned subsidiary of OncoGenex Pharmaceuticals, which is a Delaware incorporated company subject to US Federal Statutory rates of 34% for all three years presented.
For the purposes of estimating the tax rate in effect at the time that deferred tax assets and liabilities are expected to reverse, we used the furthest out available future tax rate in the applicable jurisdictions. For the years ended December 31, 2015, 2014 and 2013 the future Canadian enacted rates we used were 26%, 26%, and 25%, respectively, while for the US the future enacted rate we used was 34% for all three periods presented.
[b] At December 31, 2015, we have investment tax credits of $2.3 million (2014—$2.4 million) available to reduce future Canadian income taxes otherwise payable. We also have non-capital loss carryforwards of $100.4 million (2014—$96.3 million) available to offset future taxable income in Canada and federal net operating loss carryforwards of $151.9 million (2014—$151.1 million) to offset future taxable income in the United States.
Under Section 382 of the Internal Revenue Code of 1986, substantial changes in our ownership may limit the amount of net operating loss carryforwards and development tax credit carryforwards that could be utilized annually in the future to offset taxable income. Any such annual limitation may significantly reduce the utilization of the net operating losses and tax credits before they expire. A 382 limitation study has been undertaken but the study is not complete. The final results of this study could indicate that the U.S. losses may be materially limited; however, the amount of such limitation cannot be reasonably quantified at this time, but may be significant. In each period since our inception, we have recorded a valuation allowance for the full amount of our deferred tax asset, as the realization of the deferred tax asset is uncertain.
|
(In thousands) |
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Income taxes at statutory rates (at a rate of 34% for all periods presented) |
|
$ |
(5,712 |
) |
|
$ |
(8,922 |
) |
|
$ |
(10,829 |
) |
|
Expenses not deducted for tax purposes |
|
|
(14 |
) |
|
|
(452 |
) |
|
|
(738 |
) |
|
Effect of tax rate changes on deferred tax assets and liabilities |
|
|
(13 |
) |
|
|
(9 |
) |
|
|
(744 |
) |
|
Rate differential on foreign earnings |
|
|
689 |
|
|
|
1,445 |
|
|
|
2,003 |
|
|
Reduction (increase) in benefit of operating losses |
|
|
(32 |
) |
|
|
441 |
|
|
|
(10 |
) |
|
Reduction in the benefit of other tax attributes |
|
|
— |
|
|
|
— |
|
|
|
- |
|
|
Investment tax credits |
|
|
(297 |
) |
|
|
(357 |
) |
|
|
(347 |
) |
|
Change in valuation allowance |
|
|
5,114 |
|
|
|
7,854 |
|
|
|
10,538 |
|
|
Book to tax return adjustments |
|
|
265 |
|
|
|
— |
|
|
|
127 |
|
|
Other |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Income tax expense |
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
As a result, we have not recognized any federal or state income tax benefit in our statement of operations. The initial public offering of common stock by us in 1995 caused an ownership change pursuant to applicable regulations in effect under the Internal Revenue Code of 1986. Therefore, our use of losses incurred through the date of ownership change will be limited during the carryforward period and may result in the expiration of net operating loss carryforwards in the United States before utilization.
78
The investment tax credits and non-capital losses and net operating losses for income tax purposes expire as follows (in thousands):
|
|
|
Investment |
|
|
Net Operating |
|
|
Non-capital |
|
|||
|
|
|
Tax Credits |
|
|
Losses |
|
|
Losses |
|
|||
|
2016 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2017 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
2018 |
|
|
150 |
|
|
|
10,795 |
|
|
|
— |
|
|
2019 |
|
|
102 |
|
|
|
32 |
|
|
|
— |
|
|
2020 |
|
|
76 |
|
|
|
2,745 |
|
|
|
— |
|
|
2021 |
|
|
69 |
|
|
|
400 |
|
|
|
— |
|
|
2022 |
|
|
105 |
|
|
|
11,766 |
|
|
|
— |
|
|
2023 |
|
|
96 |
|
|
|
10,785 |
|
|
|
— |
|
|
2024 |
|
|
111 |
|
|
|
16,814 |
|
|
|
— |
|
|
2025 |
|
|
144 |
|
|
|
2,062 |
|
|
|
— |
|
|
2026 |
|
|
400 |
|
|
|
27,157 |
|
|
|
7,335 |
|
|
2027 |
|
|
173 |
|
|
|
22,225 |
|
|
|
4,949 |
|
|
2028 |
|
|
390 |
|
|
|
12,648 |
|
|
|
8,020 |
|
|
2029 |
|
|
317 |
|
|
|
4,358 |
|
|
|
(9 |
) |
|
2030 |
|
|
346 |
|
|
|
5,034 |
|
|
|
6,288 |
|
|
2031 |
|
|
608 |
|
|
|
6,200 |
|
|
|
12,121 |
|
|
2032 |
|
|
505 |
|
|
|
8,418 |
|
|
|
17,278 |
|
|
2033 |
|
|
422 |
|
|
|
2,520 |
|
|
|
23,240 |
|
|
2034 |
|
|
219 |
|
|
|
2,609 |
|
|
|
18,027 |
|
|
2035 |
|
|
328 |
|
|
|
5,342 |
|
|
|
3,120 |
|
|
|
|
$ |
4,561 |
|
|
$ |
151,910 |
|
|
$ |
100,369 |
|
In addition, we have unclaimed tax deductions of approximately $14.3 million related to scientific research and experimental development expenditures available to carry forward indefinitely to reduce Canadian taxable income of future years. We also have research and development tax credits of $2.3 million available to reduce future taxes payable in the United States. The research and development tax credits expire between 2016 and 2035.
[c] Significant components of our deferred tax assets as of December 31 are shown below (in thousands):
The potential income tax benefits relating to these deferred tax assets have not been recognized in the accounts as their realization did not meet the requirements of “more likely than not” under the liability method of tax allocation. Accordingly, a valuation allowance has been recorded and no deferred tax assets have been recognized as at December 31, 2015 and 2014.
|
|
|
2015 |
|
|
2014 |
|
||
|
Deferred tax assets: |
|
|
|
|
|
|
|
|
|
Tax basis in excess of book value of assets |
|
$ |
6,308 |
|
|
$ |
4,871 |
|
|
Non-capital loss carryforwards |
|
|
77,746 |
|
|
|
76,403 |
|
|
Research and development deductions and credits |
|
|
7,484 |
|
|
|
7,464 |
|
|
Stock options |
|
|
3,448 |
|
|
|
3,163 |
|
|
Restructuring liability |
|
|
474 |
|
|
|
(25 |
) |
|
Other |
|
|
1,627 |
|
|
|
110 |
|
|
Total deferred tax assets |
|
|
97,087 |
|
|
|
91,986 |
|
|
Valuation allowance |
|
$ |
(97,087 |
) |
|
$ |
(91,986 |
) |
[d] Under ASC 740, the benefit of an uncertain tax position that is more likely than not of being sustained upon audit by the relevant taxing authority must be recognized at the largest amount that is more likely than not to be sustained. No portion of the benefit of an uncertain tax position may be recognized if the position has less than a 50% likelihood of being sustained.
79
A reconciliation of the unrecognized tax benefits of uncertain tax positions for the year ended December 31, 2015 is as follows (in thousands):
|
|
|
Year ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Balance at January 1 |
|
$ |
2,039 |
|
|
$ |
2,007 |
|
|
$ |
1,967 |
|
|
Additions based on tax positions related to the current year |
|
|
16 |
|
|
|
32 |
|
|
|
32 |
|
|
Additions based on tax positions related to prior years |
|
|
- |
|
|
|
- |
|
|
|
8 |
|
|
Balance at December 31 |
|
$ |
2,055 |
|
|
$ |
2,039 |
|
|
$ |
2,007 |
|
As of December 31, 2015, unrecognized benefits of approximately $2.1 million, if recognized, would affect our effective tax rate, and would reduce our deferred tax assets.
Our accounting policy is to treat interest and penalties relating to unrecognized tax benefits as a component of income taxes. As of December 31, 2015 and December 31, 2014 we had no accrued interest and penalties related to income taxes.
We are subject to taxes in Canada and the U.S. until the applicable statute of limitations expires. Tax audits by their very nature are often complex and can require several years to complete.
|
Tax |
|
Years open to |
|
Jurisdiction |
|
examination |
|
Canada |
|
2008 to 2015 |
|
US |
|
2012 to 2015 |
10. COMMON STOCK
[a] Authorized
75,000,000 authorized common voting share, par value of $0.001, and 5,000,000 preferred shares, par value of $0.001.
[b] Issued and outstanding shares
At-The-Market Issuance Sales Agreement
In June 2013, we entered into an At-the-Market Issuance Sales Agreement, or Sales Agreement, with MLV & Co. LLC, or MLV, under which we may offer and sell shares of our common stock having aggregate sales proceeds of up to $25 million from time to time through MLV as our sales agent. Sales of our common stock through MLV, if any, will be made by any method permitted that is deemed an “at the market” offering as defined in Rule 415 under the Securities Act of 1933, as amended, including by means of ordinary brokers’ transactions on The NASDAQ Capital Market or otherwise at market prices prevailing at the time of sale, in block transactions, or as otherwise agreed upon by us and MLV. MLV will use commercially reasonable efforts to sell our common stock from time to time, based upon instructions from us (including any price, time or size limits or other customary parameters or conditions we may impose). We will pay MLV a commission of up to 3.0% of the gross sales proceeds of any shares of common stock sold through MLV under the Sales Agreement. We are not obligated to make any sales of common stock under the Sales Agreement. The offering of our shares of common stock pursuant to the Sales Agreement will terminate upon the earlier of (i) the sale of all common stock subject to the Sales Agreement or (ii) termination of the Sales Agreement in accordance with its terms.
On April 27, 2015, we and MLV terminated the Sales Agreement. We were not subject to any termination penalties related to termination of the Sales Agreement. Under the Sales Agreement, we offered and sold 809,214 shares of our common stock with MLV & Co. LLC. These sales resulted in gross proceeds to us of approximately $3.0 million and offering expenses of $0.1 million.
July 2014 Registered Offering
On July 2, 2014, we completed an underwritten registered offering pursuant to which we sold 5,559,866 Series A units at a price per unit of $3.48 and 1,340,538 Series B units at a price per unit of $3.47.
80
Each Series A unit consisted of one share of common stock and a Series A warrant to purchase up to one-half of one share of common stock at an initial exercise price of $4.00 per share. Each Series A warrant is exercisable at any time on or after the date of issuance until the fifth anniversary of the issuance of the Series A warrants.
Each Series B unit consisted of a Pre-Funded Series B warrant to purchase up to one share of common stock at an initial exercise price of $0.01 per share and a Series B warrant to purchase up to one-half of one share of common stock at an initial exercise price of $4.00 per share. Each Pre-Funded Series B warrant and Series B warrant is exercisable at any time on or after the date of issuance until the fifth anniversary of the issuance of the Pre-Funded Series B warrants and Series B warrants, respectively.
We received net proceeds of approximately $22.4 million, after deducting underwriting discounts and commissions and offering expenses. Gross proceeds of $24.0 million and underwriting discounts and commissions and offering expenses of $1.6 million were allocated as follows:
|
|
|
|
|
|
|
Series B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pre-funded |
|
|
Series A |
|
|
Series B |
|
|||
|
|
|
|
|
|
|
Common |
|
|
Common |
|
|
Common |
|
|||
|
|
|
Common |
|
|
Stock |
|
|
Stock |
|
|
Stock |
|
||||
|
|
|
Stock |
|
|
Warrants |
|
|
Warrants |
|
|
Warrants |
|
||||
|
Units Issued |
|
|
5,559,866 |
|
|
|
1,340,538 |
|
|
|
2,779,933 |
|
|
|
670,269 |
|
|
Gross Proceeds (in thousands) |
|
$ |
14,084 |
|
|
$ |
3,387 |
|
|
$ |
5,261 |
|
|
$ |
1,268 |
|
|
Underwriting discount and offering expense (in thousands) |
|
$ |
885 |
|
|
$ |
213 |
|
|
$ |
428 |
|
|
$ |
103 |
|
The Series A and Series B common stock warrants are classified as liabilities. The underwriting discount and offering expenses allocated to the Series A and Series B common stock warrants have been expensed in the Consolidated Statement of Loss.
The common stock and Series B prefunded common stock warrants are classified as equity. The underwriting discount and offering expenses allocated to the common stock and Series B prefunded common stock warrants have been charged against the allocated gross proceeds.
Purchase Agreement and Financing with Lincoln Park Capital
On April 30, 2015, we and Lincoln Park Capital Fund, LLC, or LPC, entered into a share and unit purchase agreement, or Purchase Agreement, pursuant to which we have the right to sell to LPC up to $18.0 million in shares of our common stock, par value $0.001 per share, subject to certain limitations and conditions set forth in the Purchase Agreement.
Pursuant to the Purchase Agreement, LPC initially purchased 956,938 Series A-1 Units at a purchase price of $2.09 per unit, with each Series A-1 Unit consisting of (a) one share of Common Stock and (b) one warrant to purchase one-quarter of a share of Common Stock at an exercise price of $2.40 per share, or Series A-1 Warrant. Each Series A-1 Warrant is exercisable six months following the issuance date until the date that is five years and six months after the issuance date and is subject to customary adjustments. The Series A-1 Warrants were issued only as part of the Series A-1 Units in the initial purchase of $2.0 million and no warrants were issued in connection with any other purchases of common stock under the Purchase Agreement.
After the initial purchase, as often as every business day over the 24-month term of the Purchase Agreement, and up to an aggregate amount of an additional $16.0 million (subject to certain limitations) of shares of common stock, we had the right, from time to time, in our sole discretion and subject to certain conditions to direct LPC to purchase up to 125,000 shares of common stock with such amounts increasing as the closing sale price of our common stock as reported on The NASDAQ Capital Market increased. The purchase price of shares of common stock pursuant to the Purchase Agreement was based on prevailing market prices of common stock at the time of sales without any fixed discount, and we controlled the timing and amount of common stock sold to LPC. In addition, we had the right to direct LPC to purchase additional amounts as accelerated purchases if on the date of a regular purchase the closing sale price of the common stock is not below $1.50 per share. As consideration for entering into the Purchase Agreement, we issued to LPC 126,582 shares of common stock; no cash proceeds were received from the issuance of these shares.
From April 30, 2015 through August 13, 2015, we offered and sold 6,814,980 shares of our common stock pursuant to our Purchase Agreement with LPC. These sales resulted in gross proceeds to us of approximately $18.0 million and offering expenses of $0.4 million. As of August 13, 2015, no further amounts remained available for sale under this offering program
Stock Option Exercises
During the year ended December 31, 2015, we issued 5,359 and 269,401 shares of common stock to satisfy stock option exercises and restricted stock unit settlements, respectively, compared with the issuance of 10,000 and 203,148 shares of common to satisfy stock option exercises and restricted stock unit settlements, respectively, for the years ended December 31, 2014. For the year ended
81
December 31, 2013, we issued 3,475 and 47,495 shares of common stock to satisfy stock option exercises and restricted stock unit settlements, respectively.
[c] Stock options
As at December 31, 2015 we had reserved, pursuant to our 2010 Performance Incentive Plan, 3,876,151 common shares for issuance upon exercise of stock options and settlement of restricted stock units by employees, directors, officers and consultants of ours, of which 1,479,221 are reserved for options currently outstanding, 640,759 are reserved for restricted stock units currently outstanding and 1,756,171 are available for future equity award grants under our 2010 Performance Incentive Plan. As of December 31, 2014 2,906,777 shares were available for equity award grants under our 2010 Performance Incentive Plan.
2010 Performance Incentive Plan
At our 2013 Annual Meeting of Stockholders held on May 24, 2013, our stockholders approved an amendment to our 2010 Performance Incentive Plan. As a result of this amendment, the 2010 Plan was further amended to provide for an increase in the total shares of common stock available for issuance under the 2010 Plan from 1,050,000 to 2,050,000. At our 2014 Annual Meeting of Stockholders held on May 29, 2014, our stockholders approved an amendment to our 2010 Performance Incentive Plan. As a result of this amendment, the 2010 Plan was amended to provide for an increase in the total shares of common stock available for issuance under the 2010 Plan from 2,050,000 to 2,800,000. At our 2015 Annual Meeting of Stockholders held on May 21, 2015, our stockholders approved an amendment to our 2010 Performance Incentive Plan. As a result of this amendment, the 2010 Plan was amended to provide for an increase in the total shares of common stock available for issuance under the 2010 Plan from 2,800,000 to 4,300,000.
Under the plan, we may grant options to purchase common shares or restricted stock units to our employees, directors, officers and consultants. The exercise price of the options is determined by our board of directors but will be at least equal to the fair value of the common shares at the grant date. The options vest in accordance with terms as determined by our board of directors, typically over three to four years for options issued to employees and consultants, and over one to three years for members of our board of directors. The expiry date for each option is set by our board of directors with a maximum expiry date of ten years from the date of grant.
Options remain outstanding under a number of share option plans that had been approved by shareholders prior to the approval of the 2010 Performance Incentive Plan: (a) the 2000 Stock Incentive Plan (2000 Plan), (b) the 2007 Performance Incentive Plan (2007 Plan) and (c) the OncoGenex Technologies Inc. Stock Option Plan (OncoGenex Technologies Plan).
ASC 718 Compensation – Stock Compensation
We recognize expense related to the fair value of our stock-based compensation awards using the provisions of ASC 718. We use the Black-Scholes option pricing model as the most appropriate fair value method for our stock options and recognize compensation expense for stock options on a straight-line basis over the requisite service period. In valuing our stock options using the Black-Scholes option pricing model, we make assumptions about risk-free interest rates, dividend yields, volatility and weighted average expected lives, including estimated forfeiture rates of the options.
The expected life was calculated based on the simplified method as permitted by the SEC’s Staff Accounting Bulletin 110, Share-Based Payment. We consider the use of the simplified method appropriate because we believe our historical stock option exercise activity may not be indicative of future stock option exercise activity because of the AFFINITY clinical data results we expect to receive in the third quarter of 2016, the structural changes to our business that may result and the potential impact of that data on our business operations and future stock option exercise activity. The expected volatility of options granted was calculated based on the historical volatility of the shares of our common stock. The risk-free interest rate is based on a U.S. Treasury instrument whose term is consistent with the expected life of the stock options. In addition to the assumptions above, as required under ASC 718, management made an estimate of expected forfeitures and is recognizing compensation costs only for those equity awards expected to vest. Forfeiture rates are estimated using historical actual forfeiture rates. These rates are adjusted on a quarterly basis and any change in compensation expense is recognized in the period of the change. We have never paid or declared cash dividends on our common stock and do not expect to pay cash dividends in the foreseeable future.
The estimated fair value of stock options granted in the respective periods was determined using the Black-Scholes option pricing model using the following weighted average assumptions:
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Risk-free interest rates |
|
|
1.76 |
% |
|
|
1.83 |
% |
|
|
1.25 |
% |
|
Expected dividend yield |
|
|
0 |
% |
|
|
0 |
% |
|
|
0 |
% |
|
Expected life |
|
5.8 years |
|
|
5.9 years |
|
|
5.8 years |
|
|||
|
Expected volatility |
|
|
63 |
% |
|
|
82 |
% |
|
|
86 |
% |
82
The weighted average fair value of stock options granted during the year ended December 31, 2015, 2014 and 2013 was $1.10, $6.52 and $8.07 per share, respectively.
The results for the periods set forth below included stock-based compensation expense in the following expense categories of the consolidated statements of loss (in thousands):
|
|
|
Years ended |
|
|||||||||
|
|
|
December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Research and development |
|
$ |
1,111 |
|
|
$ |
1,893 |
|
|
$ |
1,296 |
|
|
General and administrative |
|
|
1,217 |
|
|
|
1,967 |
|
|
|
1,538 |
|
|
Total stock-based compensation |
|
$ |
2,328 |
|
|
$ |
3,860 |
|
|
$ |
2,834 |
|
Options vest in accordance with terms as determined by our board of directors, typically over three or four years for employee and consultant grants and over one or three years for board of director option grants. The expiry date for each option is set by our board of directors with, which is typically seven to ten years. The exercise price of the options is determined by our board of directors but is at least equal to the fair value of the share at the grant date.
Stock option transactions and the number of stock options outstanding are summarized below:
|
|
|
Number of |
|
|
Weighted |
|
||
|
|
|
Optioned |
|
|
Average |
|
||
|
|
|
Common |
|
|
Exercise |
|
||
|
|
|
Shares |
|
|
Price |
|
||
|
Balance, January 1, 2013 |
|
|
805,281 |
|
|
$ |
11.34 |
|
|
Granted |
|
|
239,282 |
|
|
|
11.32 |
|
|
Expired |
|
|
(3,061 |
) |
|
|
4.11 |
|
|
Exercised |
|
|
(3,475 |
) |
|
|
3.00 |
|
|
Forfeited |
|
|
(30,536 |
) |
|
|
13.87 |
|
|
Balance, December 31, 2013 |
|
|
1,007,491 |
|
|
$ |
11.39 |
|
|
Granted |
|
|
382,097 |
|
|
|
8.97 |
|
|
Expired |
|
|
(12,169 |
) |
|
|
18.93 |
|
|
Exercised |
|
|
(10,000 |
) |
|
|
3.00 |
|
|
Forfeited |
|
|
(84,000 |
) |
|
|
12.14 |
|
|
Balance, December 31, 2014 |
|
|
1,283,419 |
|
|
$ |
10.55 |
|
|
Granted |
|
|
502,047 |
|
|
|
1.91 |
|
|
Expired |
|
|
(247,766 |
) |
|
|
2.96 |
|
|
Exercised |
|
|
(5,359 |
) |
|
|
2.69 |
|
|
Forfeited |
|
|
(53,120 |
) |
|
|
14.37 |
|
|
Balance, December 31, 2015 |
|
|
1,479,221 |
|
|
$ |
8.78 |
|
83
The following table summarizes information about stock options outstanding at December 31, 2015 regarding the number of ordinary shares issuable upon: (1) outstanding options and (2) vested options.
(1) Number of common shares issuable upon exercise of outstanding options:
|
|
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
Contractual |
|
||
|
|
|
|
|
|
|
Average |
|
|
Life |
|
||
|
Exercise Prices |
|
Number of Options |
|
|
Exercise Price |
|
|
(in years) |
|
|||
|
$1.16 - $1.54 |
|
|
8,750 |
|
|
$ |
1.17 |
|
|
|
9.93 |
|
|
$1.55 - $1.88 |
|
|
424,797 |
|
|
|
1.86 |
|
|
|
9.38 |
|
|
$1.89 - $3.04 |
|
|
115,500 |
|
|
|
2.35 |
|
|
|
9.24 |
|
|
$3.05 - $11.17 |
|
|
143,879 |
|
|
|
5.89 |
|
|
|
7.09 |
|
|
$11.18 - $11.84 |
|
|
218,147 |
|
|
|
11.78 |
|
|
|
8.14 |
|
|
$11.85 - $11.99 |
|
|
154,251 |
|
|
|
11.95 |
|
|
|
7.14 |
|
|
$12.00 - $13.06 |
|
|
136,325 |
|
|
|
12.87 |
|
|
|
6.26 |
|
|
$13.07 - $15.74 |
|
|
37,676 |
|
|
|
14.33 |
|
|
|
5.35 |
|
|
$15.75 - $16.40 |
|
|
110,250 |
|
|
|
15.97 |
|
|
|
4.96 |
|
|
$16.41 - $22.28 |
|
|
129,646 |
|
|
|
20.06 |
|
|
|
4.23 |
|
|
Total |
|
|
1,479,221 |
|
|
$ |
8.78 |
|
|
|
7.56 |
|
(2) Number common shares issuable upon exercise of vested options:
|
|
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
Weighted- |
|
|
Contractual |
|
||
|
|
|
|
|
|
|
Average |
|
|
Life |
|
||
|
Exercise Prices |
|
Number of Options |
|
|
Exercise Price |
|
|
(in years) |
|
|||
|
$1.16 - $1.54 |
|
|
547 |
|
|
$ |
1.17 |
|
|
|
9.93 |
|
|
$1.55 - $1.88 |
|
|
96,695 |
|
|
|
1.86 |
|
|
|
9.38 |
|
|
$1.89 - $3.04 |
|
|
19,042 |
|
|
|
2.44 |
|
|
|
9.05 |
|
|
$3.05 - $11.17 |
|
|
99,764 |
|
|
|
6.58 |
|
|
|
6.50 |
|
|
$11.18 - $11.84 |
|
|
107,491 |
|
|
|
11.78 |
|
|
|
8.07 |
|
|
$11.85 - $11.99 |
|
|
113,949 |
|
|
|
11.95 |
|
|
|
7.12 |
|
|
$12.00 - $13.06 |
|
|
134,044 |
|
|
|
12.87 |
|
|
|
6.26 |
|
|
$13.07 - $15.74 |
|
|
35,284 |
|
|
|
14.39 |
|
|
|
5.25 |
|
|
$15.75 - $16.40 |
|
|
110,250 |
|
|
|
15.97 |
|
|
|
4.96 |
|
|
$16.41 - $22.28 |
|
|
129,646 |
|
|
|
20.06 |
|
|
|
4.23 |
|
|
Total |
|
|
846,712 |
|
|
$ |
11.93 |
|
|
|
6.53 |
|
As at December 31, 2015, the total unrecognized compensation expense related to stock options granted was $1.8 million, which is expected to be recognized into expense over a period of approximately 2.1 years.
The estimated grant date fair value of stock options vested during the years ended December 31, 2015, 2014 and 2013 was $1.3 million, $1.9 million and $1.8 million, respectively.
The aggregate intrinsic value of options exercised was calculated as the difference between the exercise price of the stock options and the fair value of the underlying common stock as of the date of exercise. The aggregate intrinsic value of options exercised for the years ended December 31, 2015, 2014 and 2013 was $2,787, $51,100 and $34,000, respectively. At December 31, 2015, the aggregate intrinsic value of the outstanding options was $350 and the aggregate intrinsic value of the exercisable options was zero.
84
[d] Restricted Stock Unit Awards
We grant restricted stock unit awards that generally vest and are expensed over a four year period. We also grant restricted stock unit awards that vest in conjunction with certain performance conditions to certain executive officers and key employees. At each reporting date, we are required to evaluate whether achievement of the performance conditions is probable. Compensation expense is recorded over the appropriate service period based upon our assessment of accomplishing each performance provision. For the years ended December 31, 2015, 2014 and 2013, $1.1 million, $2.2 million and $1.1 million, respectively, of stock based compensation expense was recognized related to these awards.
The following table summarizes our restricted stock unit award activity during the years ended December 31, 2015, 2014 and 2013:
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
Number |
|
|
Average |
|
||
|
|
|
of |
|
|
Grant Date |
|
||
|
|
|
Shares |
|
|
Fair Value |
|
||
|
Balance, January 1, 2013 |
|
|
172,085 |
|
|
$ |
13.01 |
|
|
Granted |
|
|
255,895 |
|
|
|
11.64 |
|
|
Vested |
|
|
(50,773 |
) |
|
|
12.95 |
|
|
Forfeited or expired |
|
|
(20,618 |
) |
|
|
12.51 |
|
|
Balance, December 31, 2013 |
|
|
356,589 |
|
|
$ |
12.06 |
|
|
Granted |
|
|
814,800 |
|
|
|
6.48 |
|
|
Vested |
|
|
(199,887 |
) |
|
|
7.00 |
|
|
Forfeited or expired |
|
|
(291,301 |
) |
|
|
10.93 |
|
|
Balance, December 31, 2014 |
|
|
680,201 |
|
|
$ |
7.34 |
|
|
Granted |
|
|
249,775 |
|
|
|
1.92 |
|
|
Vested |
|
|
(269,401 |
) |
|
|
8.08 |
|
|
Forfeited or expired |
|
|
(19,816 |
) |
|
|
7.27 |
|
|
Balance, December 31, 2015 |
|
|
640,759 |
|
|
$ |
4.92 |
|
As of December 31, 2015, we had approximately $2.0 million in total unrecognized compensation expense related to our restricted stock unit awards which is to be recognized over a weighted-average period of approximately 2.2 years.
[e] Stock Warrants
The following is a summary of outstanding warrants to purchase common stock at December 31, 2015:
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
Outstanding |
|
|
Exercise |
|
|
|
||
|
|
|
and |
|
|
price per |
|
|
|
||
|
|
|
Exercisable |
|
|
Share |
|
|
Expiration Date |
||
|
(1) Series A Warrants issued in July 2014 financing |
|
|
2,779,933 |
|
|
|
4.00 |
|
|
July 2019 |
|
(2) Series B Warrants issued in July 2014 financing |
|
|
670,269 |
|
|
|
4.00 |
|
|
July 2019 |
|
(3) Series A-1 Warrants issued in April 2015 financing |
|
|
239,234 |
|
|
|
2.40 |
|
|
October 2020 |
No warrants were exercised for the year ended December 31, 2015. For the year ended December 31, 2014, all the Pre-Funded Series B warrants were exercised at a per unit price of $0.01, a total of 1,340,538 shares of common stock were issued for proceeds of $13,405. No Series A and Series B warrants from the July 2014 financing were exercised in 2014.
The Series A and Series B warrants issued in the July 2014 financing are classified as liabilities. The estimated fair value of warrants issued and classified as liabilities is reassessed at each reporting date using the Black-Scholes option pricing model. The Series A-1 Warrants issued in the April 2015 financing are classified as equity and are not reassessed for their fair value at the end of each reporting date. The following assumptions were used to value the warrants that are classified as liabilities on the following reporting dates:
|
|
|
As of |
|
|||||
|
|
|
December 31, |
|
|||||
|
Series A and Series B Warrant Valuation Assumptions |
|
2015 |
|
|
2014 |
|
||
|
Risk-free interest rates |
|
|
1.42 |
% |
|
|
1.51 |
% |
|
Expected dividend yield |
|
|
0 |
% |
|
|
0 |
% |
|
Expected life |
|
3.50 years |
|
|
4.50 years |
|
||
|
Expected volatility |
|
|
77 |
% |
|
|
63 |
% |
85
[f] Shareholder Rights Plan
We have a Shareholder Rights Plan which was adopted in July 1996 and subsequently amended in July 2002, October 2005, August 2006, and May 2008 (the “Rights Plan”). Under the Plan our Board of Directors declared a dividend of one Preferred Stock Purchase Right (Right) for each outstanding common share of OncoGenex. Subject to the Rights Plan, each Right entitles the registered holder to purchase from us one one-hundredth of a share of Series A Junior Participating Preferred Stock at an exercise price of $140, subject to adjustment. These Rights provide the holders with the right to purchase, in the event a person or group acquires 15% or more of our common stock, additional shares of our common stock having a market value equal to two times the exercise price of the Right. Pursuant to the Rights Plan, the one-for-eighteen reverse stock split caused a proportionate adjustment of the number of Rights associated with each share of common stock. Currently, eighteen Rights are associated with each share of common stock.
[g] 401(k) Plan
We maintain a 401(k) plan. Following the Arrangement, the Board of Directors of OncoGenex amended and restated the 401(k) plan whereas our securities are no longer offered as an investment option. This amendment prohibits the inclusion of our shares in the 401(k) plan, as well as any match of our shares to employee contributions.
[h] Loss per common share
The following table presents the computation of basic and diluted net loss attributable to common stockholders per share (in thousands, except per share and share amounts):
|
|
|
Years ended December 31, |
|
|||||||||
|
|
|
2015 |
|
|
2014 |
|
|
2013 |
|
|||
|
Numerator |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(16,801 |
) |
|
$ |
(26,240 |
) |
|
$ |
(31,849 |
) |
|
Denominator |
|
|
|
|
|
|
|
|
|
|
|
|
|
Weighted average number of common shares outstanding |
|
|
26,147,344 |
|
|
|
18,098,799 |
|
|
|
14,683,389 |
|
|
Basic and diluted net loss per common share |
|
$ |
(0.64 |
) |
|
$ |
(1.45 |
) |
|
$ |
(2.17 |
) |
As of December 31, 2015, 2014 and 2013 a total of 5.8 million, 7.0 million and 3.0 million options, restricted stock units and warrants, respectively, have not been included in the calculation of potential common shares as their effect on diluted per share amounts would have been anti-dilutive.
11. RELATED PARTY TRANSACTIONS
There were no related party transactions during the periods ended December 31, 2015, 2014 or 2013, and no amounts were included in accounts payable and accrued liabilities as at December 31, 2015 and 2014.
12. COMMITMENTS AND CONTINGENCIES
Teva Pharmaceutical Industries Ltd.
In December 2009, we, through our wholly-owned subsidiary, OncoGenex Technologies, entered into a Collaboration Agreement with Teva for the development and global commercialization of custirsen (and related compounds). In December 2014, we and Teva agreed to terminate the Collaboration Agreement upon entry into a Termination Agreement. In April 2015, OncoGenex Technologies and Teva entered into the Termination Agreement, pursuant to which the Collaboration Agreement was terminated and we regained rights to custirsen. Pursuant to the Termination Agreement, Teva paid to us, as advanced reimbursement for certain continuing research and development activities related to custirsen, an amount equal to $27.0 million less approximately $3.8 million, which reduction represented a hold-back amount of $3.0 million and $0.8 million for certain third-party custirsen-related development expenses incurred by Teva between January 1, 2015 and the Closing Date. Pursuant to the Termination Agreement, one half of the then remaining amount will be paid to us six months after the Closing Date, one half of the then remaining amount will be paid to us nine months after the Closing Date and the entire then remaining amount will be paid to us 12 months after the Closing Date. As of December 31, 2015, the entire amount of the holdback had been almost fully deducted by Teva for certain custirsen-related costs incurred after the Closing Date. We received a nominal amount from the remaining hold-back in October 2015, representing one half of the then remaining amount six months from the Closing Date. We expect to receive only nominal amounts from the remaining hold-back as a result of us paying for certain pre-Closing Date custirsen-related development costs on behalf of Teva.
All licenses granted by us to Teva under the Collaboration Agreement were terminated as of the Closing Date.
86
In accordance with the Termination Agreement, Teva transferred certain third-party agreements for the ENSPIRIT study and custirsen development activities to us on the Closing Date. If any additional historical third-party agreements are discovered after the Closing Date and are used to conduct the ENSPIRIT study, then Teva will use commercially reasonable effort to assign such agreements to us and will be responsible for any costs invoiced under such agreements in excess of an aggregate of $0.1 million. We will be responsible for the initial $0.1 million of costs under such agreements.
Prior to the termination of the Collaboration Agreement, Teva made upfront payments in the aggregate amount of $50.0 million. Teva also acquired $10.0 million of our common stock at a premium under a separate Stock Purchase Agreement. We were required to contribute $30.0 million in direct and indirect costs towards the clinical development plan. We fulfilled our obligation to contribute $30.0 million towards the development of custirsen. Teva was required to and did fund all additional expenses under the clinical development plan through December 31, 2014, after which date we took over responsibility for future costs following termination of our Collaboration Agreement. We do not owe, to Teva, any development milestone payments or royalty payments on sales of custirsen, if any.
Ionis Pharmaceuticals Inc. and University of British Columbia
We are obligated to pay milestone payments of up to CAD $1.6 million and $7.75 million pursuant to license agreements with UBC and Ionis, respectively, upon the achievement of specified product development milestones related to apatorsen and OGX-225 and low to mid-single digit royalties on future product sales.
In addition, we are required to pay to Ionis up to 20% of all non-royalty revenue (defined to mean revenue not based on net sales of products) we receive from third parties. In May and November 2015, we received communications from Ionis requesting payment of 30% of the $23.2 million paid by Teva under the Termination Agreement, as well as 30% of any amounts paid by Teva upon release of the $3.0 million holdback amount. On January 5, 2016, Ionis filed a lawsuit and claims that OncoGenex Technologies is in breach of the license agreement for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva in connection with the termination of the Collaboration Agreement. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the license agreement. We do not believe that any payments are due to Ionis. Under the Ionis license agreement, no payment is due to Ionis on any consideration that we receive for the reimbursement for research and development activities. The amounts paid or payable by Teva under the Termination Agreement constitute an advanced reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin, and therefore, no payments are owed to Ionis. We intend to vigorously defend the lawsuit and, based on our preliminary review, we believe we have valid defenses.
Unless otherwise terminated, the Ionis agreements for custirsen and apatorsen will continue for each product until the later of 10 years after the date of the first commercial product sale, or the expiration of the last to expire of any patents required to be licensed in order to use or sell the product, unless OncoGenex Technologies abandons either custirsen or apatorsen and Ionis does not elect to unilaterally continue development. The Ionis agreement for OGX-225 will continue into perpetuity unless OncoGenex Technologies abandons the product and Ionis does not elect to unilaterally continue development.
To facilitate the execution and performance of our prior Collaboration Agreement with Teva, we amended the license agreement with Ionis and UBC, as it pertains to custirsen, in December 2009.
The amendment to the license agreement with Ionis provides, among other things, that if we are subject to change of control with a third party, where the surviving company immediately following such change of control has the right to develop and sell the product, then (i) a milestone payment of $20.0 million will be due and payable to Ionis 21 days following the first commercial sale of the product in the United States; and (ii) unless such surviving entity had previously sublicensed the product and a royalty rate payable to Ionis by us has been established, the applicable royalty rate payable to Ionis will thereafter be the maximum amount payable under the license agreement. Any non-royalty milestone amounts previously paid will be credited toward the $20.0 million milestone if not already paid. As a result of the $10.0 million milestone payment payable to Ionis in relation to the Collaboration Agreement, the remaining amount owing in the event of change of control discussed above is a maximum of $10.0 million.
Lease Arrangements
We have an operating lease agreement for office space being used in Vancouver, Canada, which expires in September 2016.
The future minimum annual lease payments under the Vancouver lease is $62,000 in 2016.
In February 2015, we entered into an office lease with Grosvenor International (Atlantic Freeholds) Limited, or Landlord, pursuant to which we leased approximately 11,526 square feet located at 19820 North Creek Parkway, Bothell, Washington, 98011, commencing on February 15, 2015. The initial term of this lease will expire on April 30, 2018, with an option to extend the term for one approximately three-year period. Our monthly base rent for the premises will start at approximately $18,000 commencing on May 1, 2015 and will increase on an annual basis up to approximately $20,000. The Landlord has agreed to provide us with a construction
87
allowance of approximately $0.1 million. We will be responsible for 17% of taxes levied upon the building during each calendar year of the term. We delivered to the Landlord a letter of credit in the amount of $0.2 million, in accordance with the terms if the lease, which the Landlord may draw upon for base rent or other damages in the event of our default under this lease. We had the option to rent an additional 8,054 square feet before August 1, 2015. In August 2015 we exercised our expansion option for an additional 2,245 square feet of office space which commenced on August 1, 2015.
The remaining future minimum annual lease payments under the terminated Bothell lease are as follows (in thousands):
|
2016 |
|
|
267 |
|
|
2017 |
|
|
281 |
|
|
2018 |
|
|
95 |
|
|
Total |
|
$ |
643 |
|
Consolidated rent and operating expense relating to both the Vancouver, Canada and Bothell, Washington offices for years ended December 31, 2015, 2014 and 2013 was $0.9 million, $2.8 million and $2.8 million, respectively.
In February 2015, we entered into a Lease Termination Agreement with BMR pursuant to which we and BMR agreed to terminate our lease, dated November 21, 2006, as amended, for the premises located at 1522 217th Place S.E. in Bothell, Washington, or Terminated Lease, effective March 1, 2015. Under the Lease Termination Agreement, we paid BMR a $2.0 million termination fee. We may also pay BMR an additional termination fee of $1.3 million if we (i) meet the primary endpoint for our phase 3 clinical trial for the treatment of second line metastatic CRPC with custirsen and if we (ii) close a transaction or transactions pursuant to which we receive funding in an aggregate amount of at least $20.0 million. BMR drew approximately $0.1 million on our letter of credit with respect to its payment of deferred state sales tax and terminated the remaining balance of $0.2 million. BMR returned to us the security deposit under the Terminated Lease, less amounts deducted in accordance with the terms of the Terminated Lease, of $0.5 million.
With respect to the contingent payment of $1.3 million, we have assessed that the likelihood of meeting both contingent events is more likely than not. As a result, we have recognized the $1.3 million in lease termination liability on our balance sheet as at December 31, 2015.
Guarantees and Indemnifications
We indemnify our officers, directors and certain consultants for certain events or occurrences, subject to certain limits, while the officer or director is or was serving at its request in such capacity. The term of the indemnification period is equal to the officer’s or director’s lifetime.
The maximum amount of potential future indemnification is unlimited; however, we have obtained director and officer insurance that limits our exposure and may enable us to recover a portion of any future amounts paid. We believe that the fair value of these indemnification obligations is minimal. Accordingly, we have not recognized any liabilities relating to these obligations as of December 31, 2015.
We have certain agreements with certain organizations with which it does business that contain indemnification provisions pursuant to which it typically agrees to indemnify the party against certain types of third-party claims. We accrue for known indemnification issues when a loss is probable and can be reasonably estimated. There were no accruals for or expenses related to indemnification issues for any period presented.
Material Changes in Financial Condition
|
|
|
December 31, |
|
|||||
|
(in thousands) |
|
2015 |
|
|
2014 |
|
||
|
Total Assets |
|
$ |
58,209 |
|
|
$ |
56,291 |
|
|
Total Liabilities |
|
|
20,769 |
|
|
|
22,232 |
|
|
Total Equity |
|
|
37,440 |
|
|
|
34,059 |
|
The increase in assets at December 31, 2015 compared with December 31, 2014 was primarily due to an increase in cash as a result of the cash payment from Teva as an advance reimbursement for custirsen development costs associated with the Termination Agreement in 2015 and proceeds received from the financings under our purchase agreement with LPC. The decrease in liabilities at December 31, 2015 compared with December 31, 2014 is primarily due to lower clinical trial accruals associated with patient enrollment and treatment in the AFFINITY trial and our investigator sponsored trials evaluating apatorsen.
88
13. QUARTERLY FINANCIAL INFORMATION (UNAUDITED)
The following table summarizes the unaudited statements of operations for each quarter of 2015 and 2014 (in thousands, except per share amounts):
|
|
|
March 31 |
|
|
June 30 |
|
|
September 30 |
|
|
December 31 |
|
||||
|
2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Collaboration revenue |
|
$ |
1,374 |
|
|
$ |
4,025 |
|
|
$ |
6,737 |
|
|
$ |
6,024 |
|
|
Research and development |
|
|
3,673 |
|
|
|
6,545 |
|
|
|
8,303 |
|
|
|
6,587 |
|
|
General and administrative |
|
|
2,698 |
|
|
|
3,067 |
|
|
|
3,125 |
|
|
|
2,915 |
|
|
Total expenses |
|
|
6,371 |
|
|
|
9,612 |
|
|
|
11,428 |
|
|
|
9,502 |
|
|
Other income |
|
|
480 |
|
|
|
(423 |
) |
|
|
141 |
|
|
|
1,756 |
|
|
Net loss |
|
|
(4,517 |
) |
|
|
(6,010 |
) |
|
|
(4,550 |
) |
|
|
(1,722 |
) |
|
Basic and diluted net loss per share |
|
$ |
(0.20 |
) |
|
$ |
(0.26 |
) |
|
$ |
(0.16 |
) |
|
$ |
(0.06 |
) |
|
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Collaboration revenue |
|
$ |
11,731 |
|
|
$ |
4,929 |
|
|
$ |
4,803 |
|
|
$ |
5,653 |
|
|
Research and development |
|
|
16,903 |
|
|
|
9,883 |
|
|
|
9,586 |
|
|
|
9,852 |
|
|
General and administrative |
|
|
2,757 |
|
|
|
2,676 |
|
|
|
2,459 |
|
|
|
2,733 |
|
|
Restructuring gain |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(267 |
) |
|
Total expenses |
|
|
19,660 |
|
|
|
12,559 |
|
|
|
12,045 |
|
|
|
12,318 |
|
|
Other income |
|
|
(707 |
) |
|
|
615 |
|
|
|
2,335 |
|
|
|
983 |
|
|
Net loss |
|
|
(8,636 |
) |
|
|
(7,015 |
) |
|
|
(4,907 |
) |
|
|
(5,682 |
) |
|
Basic and diluted net loss per share |
|
$ |
(0.59 |
) |
|
$ |
(0.47 |
) |
|
$ |
(0.23 |
) |
|
$ |
(0.26 |
) |
14. SUBSEQUENT EVENTS
On January 5, 2016, Ionis Pharmaceuticals, Inc., formerly known as Ionis Pharmaceuticals, Inc., or Ionis, filed a lawsuit against our wholly owned subsidiary, OncoGenex Technologies Inc., or OncoGenex Technologies, in the United States District Court for the Southern District of California. Ionis claims that OncoGenex Technologies is in breach of an Amended and Restated License Agreement between Ionis and OncoGenex Technologies dated July 2, 2008, as amended, or License Agreement. Under the License Agreement, Ionis is entitled to a share of certain forms of non-royalty revenue received by OncoGenex Technologies, but is not entitled to a share of revenue received by OncoGenex Technologies for the reimbursement of research and development activities. In April 2015, we terminated a collaboration agreement with Teva Pharmaceuticals Industries Ltd. In connection with that termination, Teva paid us $23.2 million as an advance reimbursement for certain continuing research and development activities related to custirsen and certain other antisense inhibitors of clusterin. In the lawsuit, Ionis claims that OncoGenex Technologies is in breach of the License Agreement for failing to pay Ionis a share of the advance reimbursement payment from Teva and other non-monetary consideration received from Teva. Ionis seeks damages in the amount of at least $10 million and a declaratory judgment that, based on OncoGenex Technologies’ alleged breach, Ionis has the right to terminate the License Agreement. We intend to vigorously defend this matter and, based on our preliminary review, we believe we have valid defenses. However, litigation is inherently uncertain, and any judgment or injunctive relief entered against us or any adverse settlement could materially and adversely impact our business, financial condition, operating results and prospects. Because we are in the early stages of this matter, we are unable to estimate a reasonably possible range of loss, if any, that may result from this matter.
In January 2016, Scott Cormack, our Chief Executive Officer, married Michelle Griffin, a consultant to us. During 2015, we paid Ms. Griffin approximately $0.5 million, for consulting services. We also granted Ms. Griffin options to purchase 37,500 shares of common stock, and 18,750 restricted stock units in 2015. In addition, pursuant to the consulting agreement with Ms. Griffin, as at December 31, 2015, we had an accrued termination liability of approximately $0.4 million.
In February 2016, we committed to a plan to reduce operating expenses, which included a workforce reduction of 11 employees, representing approximately 27% of our employees prior to the reduction. We estimate we will incur approximately $0.4 million in cash expenditures as a result of the workforce reduction, substantially all of which will be severance costs to be paid out in in the first quarter of 2016.
89
None.
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that material information required to be disclosed in our periodic reports filed or submitted under the Exchange Act, is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Our disclosure controls and procedures are also designed to ensure that information required to be disclosed in the reports we file or submit under the Exchange Act is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate, to allow timely decisions regarding required disclosure.
We carried out an evaluation, under the supervision and with the participation of our management, including the principal executive officer and the principal financial officer, of the effectiveness of the design and operation of the disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act. Based on that evaluation, our principal executive officer and principal financial officer concluded that our disclosure controls and procedures were effective as of the end of the period covered by this Annual Report on Form 10-K.
Changes in Internal Control Over Financial Reporting
We have not made any changes to our internal control over financial reporting (as defined in Rule 13a-15(f) and 15d-15(f) under the Exchange Act) during the quarter ended December 31, 2015 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over our financial reporting, as defined in Rule 13a-15(f) under the Exchange Act. Our internal control over financial reporting is a process designed under the supervision of our principal executive and principal financial officers to provide reasonable assurance regarding the reliability of financial reporting and the preparation of our financial statements for external reporting purposes in accordance with U.S. generally accepted accounting principles.
As of December 31, 2015, management assessed the effectiveness of our internal control over financial reporting based on the framework established in “Internal Control—Integrated Framework” issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) (2013 Framework). Based on this evaluation, management has determined that our internal control over financial reporting was effective as of December 31, 2015.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
The effectiveness of our internal control over financial reporting as of December 31, 2015 has been audited by Ernst & Young LLP, an independent registered public accounting firm, as stated in their report which is included above.
Not applicable.
90
The information required hereunder is incorporated by reference from our definitive Proxy Statement to be filed within 120 days of December 31, 2015 and delivered to stockholders in connection with our 2016 Annual Meeting of Stockholders.
The information required hereunder is incorporated by reference from our definitive Proxy Statement to be filed within 120 days of December 31, 2015 and delivered to stockholders in connection with our 2016 Annual Meeting of Stockholders.
The following table sets forth certain information regarding our equity compensation plans as of December 31, 2015:
|
|
|
(a) |
|
|
(b) |
|
|
(c) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
Number of securities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
remaining available for |
|
|
|
|
|
|
Number of securities to be |
|
|
|
|
|
|
future issuance under |
|
|
||
|
|
|
issued upon exercise of |
|
|
Weighted-average |
|
|
equity compensation |
|
|
|||
|
|
|
outstanding options, |
|
|
exercise price of |
|
|
plans (excluding |
|
|
|||
|
|
|
restricted stock units, |
|
|
outstanding options, |
|
|
securities reflected in |
|
|
|||
|
Plan category |
|
warrants and rights |
|
|
warrants and rights |
|
|
column (a)) |
|
|
|||
|
Equity compensation plans approved by security holders |
|
|
2,119,980 |
|
(1) |
$ |
6.13 |
|
(1) |
1,756,171 |
|
(1) |
|
|
Equity compensation plans not approved by security holders(2) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
Total |
|
|
2,119,980 |
|
|
$ |
6.13 |
|
|
1,756,171 |
|
|
|
|
(1) |
As of December 31, 2015, we maintained the following equity compensation plans, which were approved by security holders: (a) the 2000 Stock Incentive Plan, (b) the 2007 Performance Incentive Plan, (c) the OncoGenex Technologies Amended and Restated Stock Option Plan and (d) the 2010 Performance Incentive Plan. |
The remaining information required hereunder is incorporated by reference from our definitive Proxy Statement to be filed within 120 days of December 31, 2015 and delivered to stockholders in connection with our 2016 Annual Meeting of Stockholders.
The information required hereunder is incorporated by reference from our definitive Proxy Statement to be filed within 120 days of December 31, 2015 and delivered to stockholders in connection with our 2016 Annual Meeting of Stockholders.
The information required hereunder is incorporated by reference from our definitive Proxy Statement to be filed within 120 days of December 31, 2015 and delivered to stockholders in connection with our 2016 Annual Meeting of Stockholders.
91
(1) Financial Statements
(2) All schedules are omitted because they are not required or the required information is included in the consolidated financial statements or notes thereto.
(3) Exhibits
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.1 |
|
Arrangement Agreement between the Company and OncoGenex Technologies Inc. dated May 27, 2008† |
|
DEF 14A |
|
000-21243 |
|
Annex A |
|
July 3, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.2 |
|
First Amendment to Arrangement Agreement between the Company and OncoGenex Technologies Inc. dated August 11, 2008 |
|
10-Q |
|
000-21243 |
|
2.2 |
|
November 10, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.3 |
|
Second Amendment to Arrangement Agreement between the Company and OncoGenex Technologies Inc. dated August 15, 2008 |
|
10-Q |
|
000-21243 |
|
2.3 |
|
November 10, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.1 |
|
Second Amended and Restated Certificate of Incorporation filed on May 24, 2013 |
|
8-K |
|
033-80623 |
|
3.1 |
|
May 29, 2013 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.2 |
|
Certificate of Amendment to Amended and Restated Certificate of Incorporation |
|
8-K |
|
033-80623 |
|
3.1 |
|
May 22, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.2 |
|
Fifth Amended and Restated Bylaws of OncoGenex Pharmaceuticals, Inc. |
|
10-Q |
|
033-80623 |
|
3.1 |
|
August 2, 2012 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.1 |
|
Specimen Certificate of Common Stock |
|
10-Q |
|
000-21243 |
|
4.1 |
|
November 10, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.2 |
|
Amended and Restated Rights Agreement dated as of July 24, 2002 between Sonus Pharmaceuticals Inc. and U.S. Stock Transfer Corporation |
|
8-A |
|
000-21243 |
|
2.1 |
|
July 25, 2002 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.3 |
|
First Amendment to Amended and Restated Rights Agreement dated as of October 17, 2005 between Sonus Pharmaceuticals Inc. and U.S. Stock Transfer Corporation |
|
8-A |
|
000-21243 |
|
2 |
|
October 18, 2005 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.4 |
|
Second Amendment to Amended and Restated Rights Agreement dated as of August 10, 2006 between Sonus Pharmaceuticals Inc. and U.S. Stock Transfer Corporation |
|
8-A |
|
000-21243 |
|
3 |
|
August 14, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
92
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.5 |
|
Third Amendment to Amended and Restated Rights Agreement dated May 27, 2008 between Sonus Pharmaceuticals Inc. and Computershare Trust Company, N.A. |
|
8-K |
|
000-21243 |
|
4.1 |
|
May 30, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.6 |
|
Form of Warrant to Purchase Common Stock |
|
8-K |
|
033-80623 |
|
4.1 |
|
October 19, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.7 |
|
Form of Series A Warrant |
|
8-K |
|
033-80623 |
|
4.1 |
|
June 27, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.8 |
|
Form of Series A-1 Warrant |
|
8-K |
|
033-80623 |
|
4.1 |
|
April 30, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.9 |
|
Form of Pre-Funded Series B Warrant |
|
8-K |
|
033-80623 |
|
4.2 |
|
June 27, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.10 |
|
Form of Series B Warrant |
|
8-K |
|
033-80623 |
|
4.3 |
|
June 27, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.1 |
|
Sonus Pharmaceuticals, Inc. 2000 Stock Incentive Plan (the “2000 Plan”)†† |
|
10-Q |
|
000-21243 |
|
10.41 |
|
August 14, 2000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.2 |
|
First Amendment to Sonus Pharmaceuticals, Inc. 2000 Plan†† |
|
10-Q |
|
000-21243 |
|
10.23 |
|
November 8, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.3 |
|
Form of Sonus Pharmaceuticals, Inc. Stock Option Agreement (pertaining to the 2000 Plan)†† |
|
10-Q |
|
000-21243 |
|
10.42 |
|
August 14, 2000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.4 |
|
Sonus Pharmaceuticals, Inc. 2007 Performance Incentive Plan (the “2007 Plan”)†† |
|
DEF 14A |
|
000-21243 |
|
Appendix A |
|
April 3, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.5 |
|
Form of Sonus Pharmaceuticals, Inc. Stock Option Agreement (pertaining to the 2007 Plan)†† |
|
10-Q |
|
000-21243 |
|
10.1 |
|
November 9, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.6 |
|
Form of Sonus Pharmaceuticals, Inc. Restricted Stock Purchase Agreement under the 2007 Plan†† |
|
10-Q |
|
000-21243 |
|
10.2 |
|
November 9, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.7 |
|
OncoGenex Technologies Inc. Amended and Restated Stock Option Plan†† |
|
F-1 |
|
333-139293 |
|
10.1 |
|
December 13, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.8 |
|
Stock Option Assumption, Amending and Confirmation Agreement dated as of August 21, 2008 between the Company and OncoGenex Technologies Inc.†† |
|
S-8 |
|
333-153206 |
|
4.2 |
|
August 26, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.9 |
|
Form of OncoGenex Pharmaceuticals, Inc 2010 Stock Option Agreement†† |
|
8-K |
|
033-80623 |
|
10.1 |
|
June 14, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.10 |
|
Form of OncoGenex Pharmaceuticals, Inc. 2010 Restricted Stock Purchase Agreement†† |
|
8-K |
|
033-80623 |
|
10.2 |
|
June 14, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.11 |
|
Form of OncoGenex Pharmaceuticals, Inc. 2010 Restricted Stock Unit Agreement†† |
|
10-Q |
|
033-80623 |
|
10.2 |
|
November 3, 2011 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.12 |
|
OncoGenex Pharmaceuticals, Inc. Short Term Incentive Awards Program†† |
|
8-K |
|
033-80623 |
|
10.1 |
|
April 2, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.13 |
|
Agreement and Consent Form (related to the Short Term Incentive Awards Program)†† |
|
8-K |
|
033-80623 |
|
10.2 |
|
April 2, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.14 |
|
OncoGenex Pharmaceuticals, Inc. 2010 Performance Incentive Plan, as amended and restated†† |
|
DEF 14A |
|
033-80623 |
|
A |
|
April 16, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.15 |
|
Form of Indemnification Agreement for Officers and Directors of the Company†† |
|
S-1 |
|
33-96112 |
|
10.19 |
|
September 25, 1995 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
93
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.16 |
|
Form of Indemnification Agreement between OncoGenex Technologies Inc. and each of Scott Cormack and Cindy Jacobs†† |
|
F-1 |
|
333-139293 |
|
10.7 |
|
December 13, 2006 |
|
|
|
10.17 |
|
Form of Indemnification Agreement between OncoGenex Technologies Inc. and Neil Clendeninn†† |
|
F-1 |
|
333-139293 |
|
10.8 |
|
December 13, 2006 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.18 |
|
Employment Agreement between OncoGenex Technologies Inc. and the Company and Scott Cormack dated as of November 4, 2009†† |
|
10-Q |
|
033-80623 |
|
10.25 |
|
November 5, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.19 |
|
Employment Agreement between the Company and Cindy Jacobs dated as of November 3, 2009†† |
|
10-Q |
|
033-80623 |
|
10.27 |
|
November 5, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.20 |
|
Employment Agreement between OncoGenex Pharmaceuticals, Inc. and John Bencich†† |
|
8-K |
|
033-80623 |
|
10.1 |
|
August 7, 2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.21 |
|
Amended and Restated License Agreement effective as of July 2, 2008 by and between OncoGenex Technologies Inc. and Isis Pharmaceuticals, Inc. (OGX-011)* |
|
10-K |
|
033-80623 |
|
10.36 |
|
March 11, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.22 |
|
Letter Agreement Regarding Certain Sublicense Consideration for OGX-011 between OncoGenex Technologies Inc. and Isis Pharmaceuticals, Inc. dated December 18, 2009 |
|
10-K |
|
033-80623 |
|
10.36 |
|
March 8, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.23 |
|
Amendment No. 1 to Amended and Restated License Agreement between OncoGenex Technologies Inc. and Isis Pharmaceuticals, Inc. dated December 19, 2009 (OGX-011)* |
|
10-K |
|
033-80623 |
|
10.37 |
|
March 8, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.24 |
|
License Agreement between OncoGenex Technologies Inc. and the University of British Columbia effective as of November 1, 2001, and Amending Agreement dated as of August 30, 2006 (OGX-011)* |
|
F-1, Amendment No. 1 |
|
333-139293 |
|
10.13 |
|
January 29, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.25 |
|
Second Amending Agreement and Consent as of August 7, 2008 between the University of British Columbia and OncoGenex Technologies Inc. (OGX-011) |
|
10-Q |
|
000-21243 |
|
2.3 |
|
November 10, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.26 |
|
Third Amending Agreement to the License Agreement between OncoGenex Technologies Inc and the University of British Columbia dated as of December 20, 2009 (OGX-011)* |
|
10-K |
|
033-80623 |
|
10.40 |
|
March 8, 2010 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.27 |
|
Collaboration and License Agreement between OncoGenex Technologies Inc. and Isis Pharmaceuticals, Inc. effective as of January 5, 2005 (OGX-427)* |
|
F-1, Amendment No. 1 |
|
333-139293 |
|
10.11 |
|
January 29, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.28 |
|
License Agreement between OncoGenex Technologies Inc. and the University of British Columbia effective as of April 5, 2005, and Amending Agreement dated as of August 30, 2006 (OGX-427)* |
|
F-1, Amendment No. 1 |
|
333-139293 |
|
10.14 |
|
January 29, 2007 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
94
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.29 |
|
Second Amending Agreement as of August 7, 2008 between the University of British Columbia and OncoGenex Technologies Inc. (OGX-427) |
|
10-Q |
|
000-21243 |
|
10.40 |
|
November 10, 2008 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.30 |
|
Termination Agreement between OncoGenex Technologies Inc. and Teva Pharmaceutical Industries Ltd.* |
|
10-Q |
|
033-80623 |
|
10.2 |
|
August 13, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.31 |
|
Office Lease by and between Grosvenor International (Atlantic Freeholds) Limited and OncoGenex Pharmaceuticals, Inc., dated February 11, 2015 |
|
8-K |
|
033-80623 |
|
10.1 |
|
February 12, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.32 |
|
Lease Termination Agreement by and between BMR-217th Place LLC and OncoGenex Pharmaceuticals, Inc., dated February 11, 2015 |
|
8-K |
|
033-80623 |
|
10.2 |
|
February 12, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.33 |
|
Purchase Agreement, dated as of April 30, 2015, by and between OncoGenex Pharmaceuticals, Inc. and Lincoln Park Capital Fund, LLC |
|
8-K |
|
033-80623 |
|
10.1 |
|
April 30, 2015 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21.1 |
|
Subsidiaries of the Registrant |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23.1 |
|
Consent of Ernst & Young LLP |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24.1 |
|
Power of Attorney (included on the signature page hereto) |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.1 |
|
Certification of Chief Executive pursuant to Rule 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.2 |
|
Certification of Chief Financial Officer pursuant to Rule 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.1 |
|
Certification of Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002** |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.2 |
|
Certification of Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002** |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.INS |
|
XBRL Instance Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.SCH |
|
XBRL Taxonomy Extension Schema Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.LAB |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
95
|
Exhibit |
|
Description |
|
Incorporated by Reference |
|
Filed/ |
||||||
|
|
|
Form |
|
File No. |
|
Exhibit |
|
Filing Date |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
|
|
|
|
|
|
X |
|
† |
Schedules and similar attachments to the Arrangement Agreement have been omitted pursuant to Item 601(b)(2) of Regulation S-K. The Company will furnish supplementally a copy of any omitted schedule or similar attachment to the SEC upon request. |
|
†† |
Indicates management contract or compensatory plan or arrangement. |
|
* |
Confidential portions of this exhibit have been omitted and filed separately with the Commission pursuant to an application for Confidential Treatment under Rule 24b-2 promulgated under the Securities Exchange Act of 1934, as amended. |
|
** |
The certifications attached as Exhibits 32.1 and 32.2 accompany to this Annual Report on Form 10-K pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, and shall not be deemed filed for purposes of Section 18 of the Securities Exchange Act of 1934, as amended. |
96
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this Report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
|
|
|
ONCOGENEX PHARMACEUTICALS, INC. |
||
|
|
|
|
|
(Registrant) |
||
|
|
|
|
|
|||
|
Date: March 9, 2016 |
|
|
|
By: |
|
/s/ SCOTT CORMACK |
|
|
|
|
|
|
|
Scott Cormack |
|
|
|
|
|
|
|
President and Chief Executive Officer |
Power of Attorney
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Scott Cormack and John Bencich, jointly and severally, as such person’s attorneys-in-fact, each with the power of substitution, for such person in any and all capacities, to sign any amendments to this Annual Report on Form 10-K, and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact, or his substitute or substitutes, may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
By: /s/ SCOTT CORMACK |
|
President and Chief Executive Officer |
|
Date: March 9, 2016 |
|
Scott Cormack |
|
|
|
|
|
|
|
|
||
|
By: /s/ JOHN BENCICH |
|
Chief Financial Officer |
|
Date: March 9, 2016 |
|
John Bencich |
|
|
|
|
|
|
|
|
||
|
By: /s/ JACK GOLDSTEIN |
|
Chairman of the Board and Director |
|
Date: March 9, 2016 |
|
Jack Goldstein |
|
|
|
|
|
|
|
|
||
|
By: /s/ NEIL CLENDENINN |
|
Director |
|
Date: March 9, 2016 |
|
Neil Clendeninn |
|
|
|
|
|
|
|
|
||
|
By: /s/ MARTIN MATTINGLY |
|
Director |
|
Date: March 9, 2016 |
|
Martin Mattingly |
|
|
|
|
|
|
|
|
||
|
By: /s/ H. STEWART PARKER |
|
Director |
|
Date: March 9, 2016 |
|
H. Stewart Parker |
|
|
|
|
|
|
|
|
||
|
By: /s/ DAVID SMITH |
|
Director |
|
Date: March 9, 2016 |
|
David Smith |
|
|
|
|
97